Table of contents
Table of Contents
Message from the Editor
Steve Elias, MD
Pelvic Venous Disease
Chronic Pelvic Pain is a Common Complaint in a Gynecologist’s Practice
Charles E. Miller, MD, FACOG
Drug Therapy for Pelvic Venous Disorders: Where Do We Stand?
Monika Gloviczki, MD
Evaluation of Pelvic Vein Reflux by Ultrasound
Nicos Labropoulos, MD
SVP for Dummies
Mark Meissner, MD
Technical Tips for Pelvic Venography
John White, MD
Open Surgical Options for Iliac Vein Compression in an Endovascular Age
Khanjan H. Nagarsheth, MD, MBA, FACS
Deep Vein/Pelvic Scientific Session at AVF 2026: Emerging Insights
Misaki Kiguchi, MD
Tips for Coil Occlusion of the Ovarian Vein
Patrick Muck, MD
AVF Updates & Membership News
Embolize Trial
Gloria Salazar, MD
Delivering on a Promise: AVF and the C-TRACT Trial
Suresh Vedantham, MD
Save the Date—and Bring Your Best to Nashville! AVF Abstract Submissions are Open
Juan Carlos Jimenez, MD and Sheila Blumberg, MD
APP Abstracts Session at AVF2027: Submit your abstract today!
Kathleen Ozsvath, MD and Karen Bauer, NP
Scholarship Opportunities Available for the AVF Venous Early Career Course
Karem Harth, MD
New Members: Welcome to the AVF!
March/April 2026
Leadership
Korn Ferry Article Feature: “Something to Believe In”
Gary Burnison, CEO
EDITOR-IN-CHIEF
Steve Elias, MD
EXECUTIVE EDITOR
John Forbes, MBA
MANAGING EDITOR
Allie Sherrill
COVER ARTIST
Christine Rataj
PUBLICATION DESIGNER
Anthony Eaves
Editor’s Letter

Steve Elias, MD
President Elect, The American Venous Forum
Chair, AVF Newsletter Committee
Grow Up and Ring Them Bells
I didn’t know what pueri aeterni meant. And I could have just continued to read on. But it bothered me. I could guess but why do that? The writer, Maureen Dowd, certainly, purposely, used those words to make a point. Her article was about AI and the scary things that are happening and could happen. Her sentence read, ‘The pueri aeterni of Silicon Valley have….”. So, to Google I went. The answer machine. I could have used ChatGPT or Claude or any other AI platform. I guess I am old school; Google it was. Pueri aeterni: the eternally youthful. Jung defined a pueri aeternus as a person, usually a man, who remains in an adolescent mindset well into adulthood. As with almost anything there are positives and negatives about being pueri aeterni. I think Maureen Dowd was not depicting the “frat boys” of Silicon Valley in a positive light. One needs to be a grown-up to understand the nuances of AI. I’ll be honest, the AI thing is overwhelming. To me, the more I read about it, the more confused I feel. The good and bad are both equally scary.
But scary is not what we strive for in Vein Specialist. Our goals are information, education, and collaboration. In this issue we cover a lot of education and information regarding pelvic venous disease. Our experts discuss diagnosis, crossover symptomatology, treatment, and simplified understanding of the SVP classification system. Read it; it is not scary. Regarding collaboration, we also cover 2 trials: C-TRACT and EMBOLIZE. Two very important ones. Finally, an important educational course is happening, the inaugural Pelvic Venous Summit. The Pelvic Venous Summit has taken a lot of work to develop and we need this education now. You need to think about these patients whether you ultimately treat them or not. Attend and give it some thought.
But I never thought much about bells, kind of took them for granted: church bells. The sound harkens back many centuries. Bells would mark daily time and signal important events. In Europe during World War II many went silent. The Nazis confiscated almost 175,000. It wasn’t the sound that they disliked; it was the metal, copper and tin, that they did like. Melted them down to make weapons. Very nasty. The decree by Hermann Göring was “Reclaiming All Bells For War Purposes.” Quite presumptive. When something is reclaimed it implies it was once yours and not someone else’s. Well, Hermann always did have an egocentric outlook on life.
After the war, campanology and campanologists to the rescue. The bells needed replacing. They encouraged bell foundries to make a better bell. Just as new, improved technology enters the vein world, so it was with the bell world. The new bells sounded better, lasted longer, and even took on new shapes. Necessity is the mother of invention. Bells have never sounded or looked better. And research about bells is still going on as research support by the AVF is always going on. Professor of Campanology Percival Price from the University of Michigan (are we surprised that he is from the University of Michigan?) has been involved. Do you realize how much good venous research emanates from the University of Michigan? But I digress. Dr Price and others like Andrea McCready used electronic oscillator instrumentation to create a database of the tonal properties of the surviving bells to be able to make better bells. Bell-making is booming. AI is booming. AVF is booming. This issue of Vein Specialist shows you how much.. So read this issue, grow up, and ring them bells.
Chronic Pelvic Pain is a Common Complaint in a Gynecologist’s Practice
Charles E. Miller, MD, FACOG
Professor, Department of Obstetrics and Gynecology, Wake Forest University Medical School President, CCRM Fertility and Gynecologic Surgeons of Illinois Director, Minimally Invasive Gynecologic Surgery, Advocate Lutheran General Hospital
Chronic pelvic pain is often a disruptive concern that significantly reduces the quality of life of the affected woman. Diagnostic workup generally includes not only evaluation of such potential gynecologic problems as endometriosis, adenomyosis, uterine fibroids, and ovarian cysts, but non-gynecologic problems such as irritable bowel syndrome, interstitial cystitis, and pelvic floor myalgia. This range of testing can lead to a multidisciplinary approach including gynecologists, gastroenterologists, urologists/urogynecologists, and pelvic floor therapists. This regimen provides pain relief to many women affected with chronic pelvic pain.
Over 10 million people in the United States are impacted by debilitating pelvic pain.
However, despite overall treatment success and knowing this multimodal approach, many of our patients remain in pain. It is this exact patient who may suffer with a pelvic venous disease (PVD) disorder. According to the literature, the etiology of upwards of 30% of women with chronic pelvic pain is pelvic venous disease. Despite this, most gynecologists are unaware of the impact of PVD on chronic pelvic pain, the workup to diagnose the disorder, nor the treatment armamentarium. We as gynecologists, the physicians, generally initiate the workup of chronic pelvic pain and manage referrals. We have all but overlooked the evaluation of venous disease and are unaware of the steps necessary to establish the diagnosis and subsequent referral to vascular surgery to discuss treatment options. This lack of understanding must change. Timely referral must be established for the diagnosis and treatment.
With the life expectancy for women increasing more rapidly than their male counterparts, and the potential diagnosis of pelvic venous disease at a very young age, as well as the potential ramifications of subsequent pregnancy on PVD, it is imperative that treatment regimens be individualized to fit the clinical situation. A clear understanding of the cause of the venous disease must be coupled with a best practices approach to the treatment plan, appropriately incorporating the potential impact of reproduction and on reproduction. Of course, this treatment plan must be incorporated into the multidisciplinary course of care.
To address the obvious need to provide a pathway of care in the diagnosis and treatment of PVD, The American Venous Forum has organized an essential and unique multidisciplinary conference to address the care of women with chronic pelvic pain secondary to PVD. Bringing together vascular specialists, gynecologists, interventional radiologists, and specialists in physical therapy/rehabilitation, the ultimate conference goal is to foster a better understanding of chronic pelvic pain and PVD in women by promoting medical specialists who care for these women, both in terms of diagnosis and treatment. This conference will surely serve as a starting point of improved collaboration among the specialists and thus provide an important educational endeavor.
See you in Chicago!

PeVD Summit Faculty:
- Rabih Chaer, MD, MSc
- Richard Cockrum, MD
- Stephen Daugherty, MD, RVT
- Alun Davies, MA DM FRCS FHEA FEBVS FACPh FLSW FMedSci
- Sergey Gavrilov, MD, PhD
- Kathleen Gibson, MD FACS
- Peter Gloviczki, MD, PhD
- Karem Harth, MD, MHS
- Houman Jalaie, MD, PhD
- Aleksandra Jaworucka-Kaczorowska, MD, PhD
- Arjun Jayaraj, MD, FACS
- Neil Khilnani, MD
- Lisa Laurenzana, MD
- Mark Meissner, MD
- Charles Miller, MD
- Mireille Astrid Moise, MD
- Kathleen Ozsvath, MD
- Peter J. Pappas, MD
- Judith Regensteiner, PhD
- Fabio Rossi, MD, PhD
- Julianne Stoughton, MD
- John V. White, MD
- Suman Wasan, MD, MS
- Gaurav Lakhanpal
- Kush Desai, MD, FSIR, FSVM
- Ruth Bush, MD, JD, MPH
Drug Therapy for Pelvic Venous Disorders: Where Do We Stand?

Monika L. Gloviczki, MD, PhD
Research Fellow, Emeritus, Department of Internal Medicine and Gonda Vascular Center, Mayo Clinic, Rochester, MN; VASA LLC, Scottsdale, AZ
Pelvic venous disorders (PeVD) are increasingly recognized as a meaningful contributor to chronic pelvic pain (CPP), a condition affecting up to a quarter of women worldwide.1 While interventional treatments such as embolization are often highlighted,2 pharmacologic therapy—particularly venoactive drugs (VADs)—offers a valuable, low-risk option for symptom control, especially in patients who are unwilling to undergo or are not candidates for procedures or who are awaiting intervention.
VADs are well established for chronic venous disease of the lower extremities and appear relevant in pelvic venous pathology, where venous hypertension, inflammation, and microcirculatory dysfunction play central roles.
In a recent systematic review that evaluated VADs therapy to alleviate symptoms of chronic pelvic pain of venous origin,3 micronized purified flavonoid fraction (MPFF), a combination of diosmin and hesperidin fraction, was the most studied pharmacologic agent.
Clinical evidence suggests that MPFF significantly reduces pelvic pain. Across multiple studies involving women with venous-origin CPP, treatment with MPFF (typically 1000 mg daily for 2–6 months) led to consistent reductions in pain scores, often measurable within 2–3 weeks of initiation. Improvements were also observed in associated symptoms such as pelvic heaviness and dyspareunia, as well as in disease-specific quality-of-life measures like the Pelvic Varicose Vein Questionnaire (PVVQ).
In more severe cases, an initial higher dose (2000 mg daily) is followed by a lower dose maintenance therapy (1000 mg daily). Response may be attenuated in patients with combined pelvic and ovarian vein reflux compared with those with isolated pelvic venous insufficiency.
Limited physiologic data suggest additional benefits, including improved venous flow, reduced vein diameter, and decreased pelvic congestion on imaging.
Safety is a key advantage of VADs therapy. Reported adverse effects are infrequent and typically mild—most commonly transient gastrointestinal discomfort. Large-scale data from venous disease populations reinforce a favorable safety profile, with no meaningful drug–drug interactions identified in routine clinical use. This contrasts with hormonal therapies (eg, GnRH agonists, medroxyprogesterone), which use is limited because of metabolic and hypoestrogenic side effects.
Additional information comes from the VENOTREAT randomized, open-label study, which demonstrates that therapies with diosmin 600 mg or a non-micronized diosmin–hesperidin combination (1000 mg) also improve symptoms in PeVD, although MPFF appears to provide faster and greater relief.4
The current evidence base is limited by small sample sizes, variable diagnostic criteria, and methodologic heterogeneity. High-quality randomized trials are needed to define optimal dosing, treatment duration, and patient selection.
References
- Ahangari A. Prevalence of chronic pelvic pain among women: an updated review. Pain Physician 2014; 17: E141–147.
- Antignani PL, Lazarashvili Z, Monedero JL, et al. Diagnosis and treatment of pelvic congestion syndrome: UIP consensus document. Int Angiol 2019; 38: 265–283. 20190724. DOI: 10.23736/S0392-9590.19.04237-8.
- Gloviczki ML, Demetres MR, Salazar G, et al. Venoactive drugs for venous origin chronic pelvic pain in women: A systematic review. Phlebology 2025: 2683555251411027. 20251223. DOI: 10.1177/02683555251411027.
- Gavrilov SG, Moskalenko YP, Grishenkova AS, et al. Venoactive drug treatment for patients with pelvic varicose veins: Results of the single-center, randomized, open-label study (VENOTREAT). Vasc Med 2025; 30: 590–598. 20250825. DOI: 10.1177/1358863X251362200.
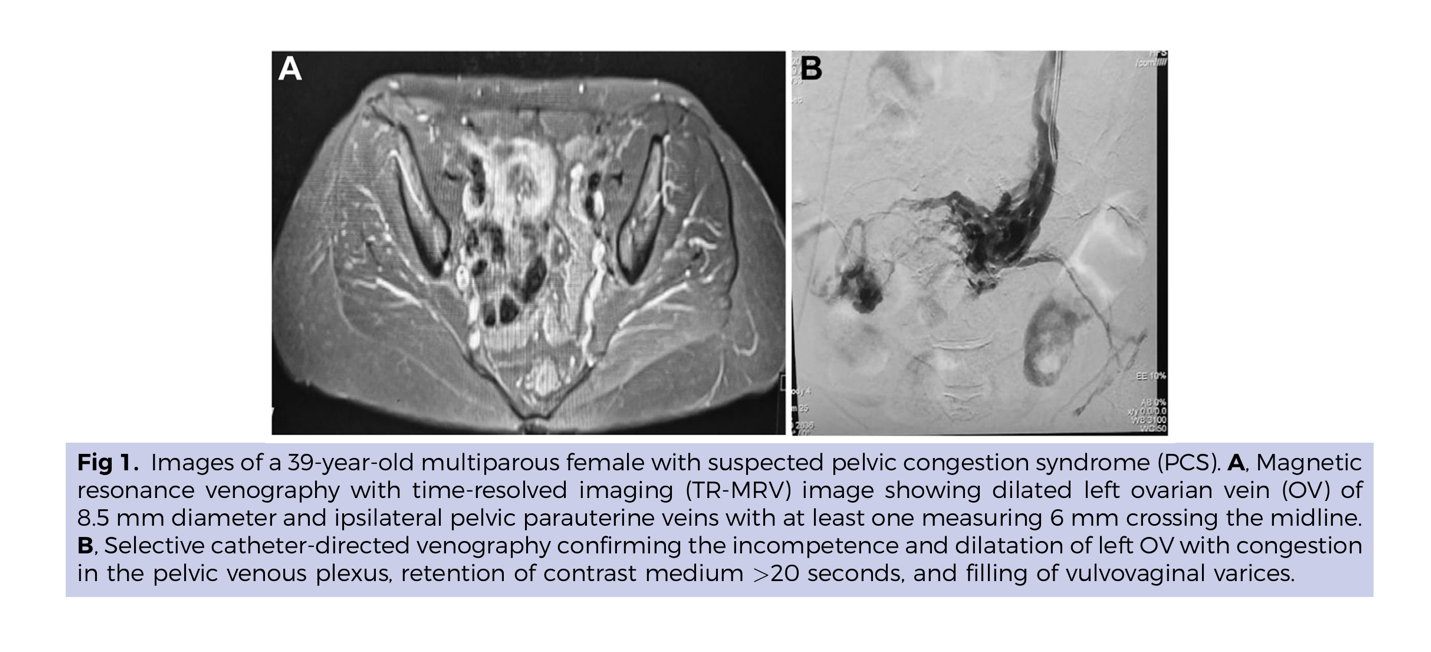
Figure from: Shahat M, Abdelbaqy OMA, AbdelHakam AM, Ali SH, and Attalla K. Can cross-sectional imaging replace diagnostic venography in pelvic venous disorder (PeVD)?
J Vasc Surg Venous Lymphat Disord 2023 Dec 20;12(2):101724. doi: 10.1016/j.jvsv.2023.101724
Evaluation of Pelvic Vein Reflux by Ultrasound

Nicos Labropoulos, PhD, RVT
Professor of Surgery and Radiology Director, Vascular Laboratory Stony Brook Medicine Stoney Brook, New York
Pelvic vein reflux is an underdiagnosed cause of chronic pelvic pain, frequently seen in multiparous women.1 Ultrasound is very important in the initial evaluation due to its accessibility, noninvasive nature, and ability to provide real-time hemodynamic information.2,3
The pelvic veins can be evaluated by ultrasound in 3 ways: transabdominal, transvaginal, and transperineal. Transabdominal ultrasound is used to evaluate the inferior vena cava, iliac, renal, ovarian, trans- and periuterine veins. It can demonstrate both reflux and obstruction and provide dynamic imaging by changing the patient position. The test sometimes may be limited by bowel gas and obesity. However, most patients with pelvic reflux are leaner and the imaging is relatively easy to perform (Figure 1).4 Transvaginal ultrasound offers good differential diagnosis for other pathologies and has great resolution for part of the iliac veins, the distal ovarian veins, and the trans- and periuterine veins. The issues with this method are imaging veins in the abdominal area. The transperineal approach in the standing position offers the best evaluation for the trans- and periuterine veins and the tributaries of the internal iliac vein. At the same time, the veins in the pelvic floor and the connections with the lower limb veins can also be evaluated. It is done in a physiologic position, where the veins have their largest diameter with a linear transducer that offers the best imaging resolution. A combination of the above tests provides the most complete information to decide how to manage such patients. A limitation of all 3 methods is the operator’s experience.
Key sonographic findings include dilated and tortuous veins, the presence of reflux and its duration, vein obstruction due to extrinsic compression or chronic post-thrombotic changes and collateral veins. Dynamic flow patterns can be easily assessed thus facilitating diagnosis. Overall, ultrasound is an important method for evaluating patients with pelvic vein disorders. It is cost-effective and can guide clinicians to optimize the management of such patients.
References
- Meissner MH, Khilnani NM, Labropoulos N, et al. The Symptoms-Varices-Pathophysiology classification of pelvic venous disorders: A report of the American Vein & Lymphatic Society International Working Group on Pelvic Venous Disorders. J Vasc Surg Venous Lymphat Disord. 2021;9:568-584.
- Labropoulos N, Jasinski PT, Adrahtas D, Gasparis AP, Meissner MH. A standardized ultrasound approach to pelvic congestion syndrome. Phlebology. 2017;32:608-619.
- Fernandes FF, Storino J, Barros FS, Silva MB, Oliveira NC, Tavares IR. Transvaginal ultrasound approach for diagnosing pelvic venous disorders. J Vasc Surg Venous Lymphat Disord. 2025;13:102286.
- Nanavati R, Jasinski P, Adrahtas D, Gasparis A, Labropoulos N. Correlation between pelvic congestion syndrome and body mass index. J Vasc Surg. 2018;67:536-541.
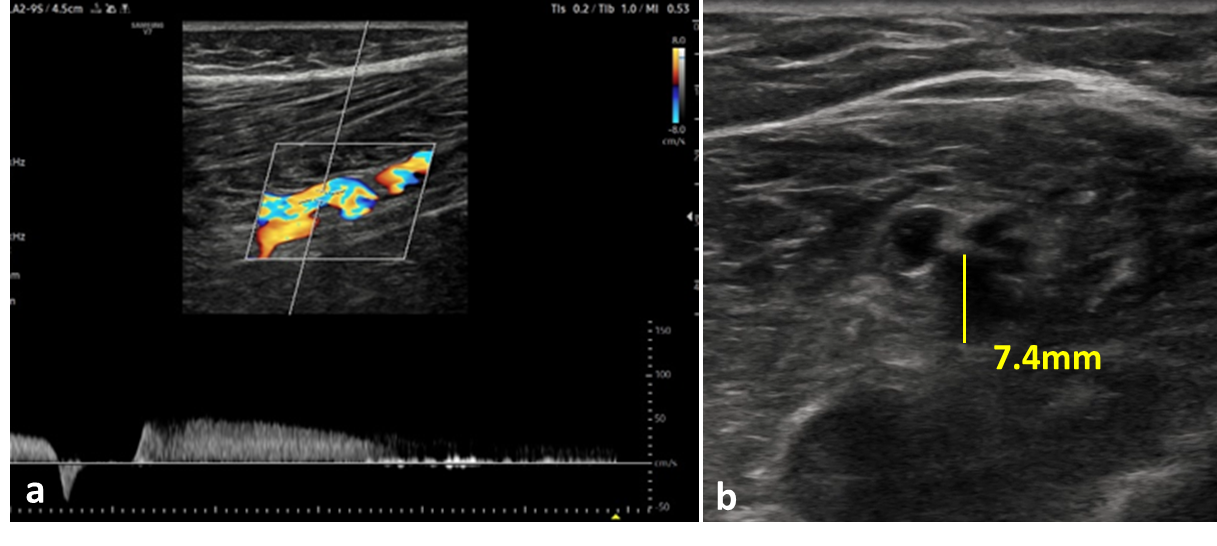
Figure 1. Left ovarian vein reflux. a. The vein is dilated and tortuous with retrograde flow. b. The diameter of the vein proximally measured 6mm and distally 7.4mm.
SVP for Dummies
Mark Meissner, MD
Peter Gloviczki Emeritus Professor of Venous & Lymphatic Disorders University of Washington School of Medicine
The CEAP classification for lower extremity venous disease has fostered effective communication among providers and provides a framework for conducting clinical research. Unfortunately, no such paradigm has existed for pelvic venous disorders. We continue to use historic nomenclature (“May-Thurner,” Nutcracker,” and “Pelvic Congestion” syndromes) based on descriptions of the underlying anatomy, which does not account for the complex symptomatology, anatomy and hemodynamics of the pelvic venous circulation. This leads to errors in diagnosis and management as well as making it difficult to conduct clinical research.
The SVP–Symptoms (S), Varices (V), and Pathophysiology (P) classification—aims to provide a comprehensive, structured framework to facilitate effective communication and identify uniform patient populations for research. The classification was modeled after and is complementary to the CEAP classification. Although designation of the involved anatomy and underlying pathophysiology is similar to CEAP, the “S” component is symptom-based while the “C” component of CEAP is sign-based. Like CEAP, it is important to recognize that SVP is a discriminative instrument, designed to categorize patients into groups with similar clinical features, natural histories, and response to treatment, rather than an evaluative instrument designed to measure severity and its longitudinal change over time.
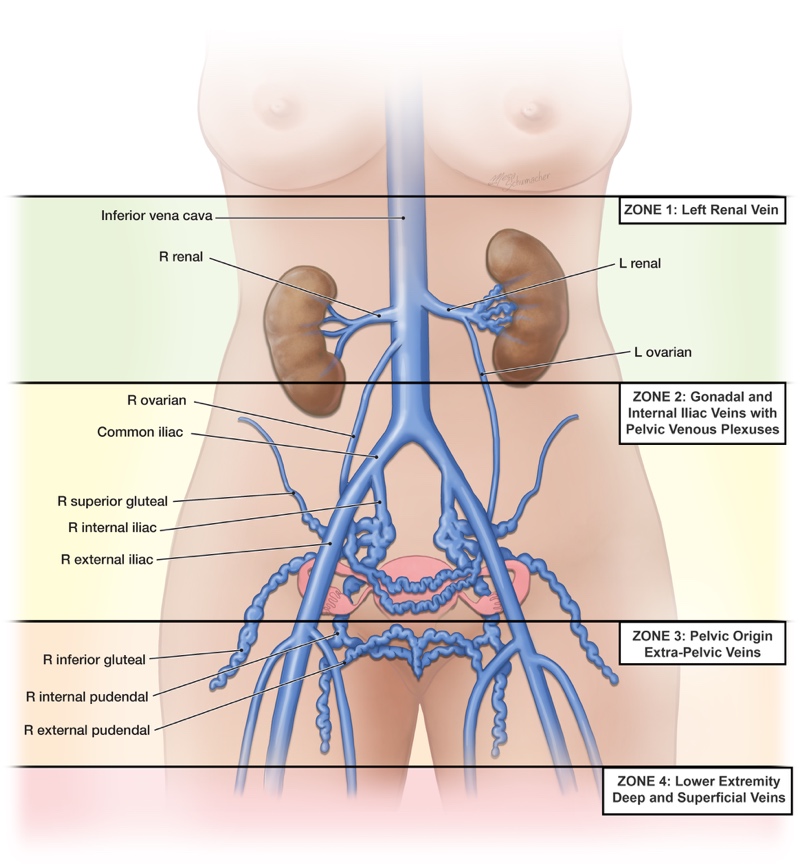
In defining subscripts for the symptoms (S) and varices (V) domains of SVP, the pelvic venous circulation is divided into 4 anatomic regions based on the primary drainage pathways and associated venous reservoirs. Increased venous pressure is transmitted to these reservoirs, leading to the development of varices and associated symptoms. Zone 1 is drained primarily by the left renal vein; is associated with renal symptoms of flank pain and hematuria; and. in uncompensated obstruction, varices in the renal hilum. Zone 2 includes the pelvic drainage pathways of the ovarian and internal iliac veins. Symptoms include chronic pelvic pain in females with varices developing in the pelvic venous plexuses. Zone 3 represents the transitional veins exiting through the pelvic escape points and includes vulvar and scrotal varices as well as venous claudication. Zone 4 includes the major superficial and deep veins of the lower extremity and is classified with CEAP, not SVP. The involved zones are designated as subscripts to “S” and “V.” For example, venous-origin chronic pelvic pain due to pelvic varices (zone 2) would be designated as S2V2, while symptomatic vulvar varices (zone 3) would be designated as S3aV2,3a (both pelvic and pelvic-origin extra-pelvic varices).
The pathophysiology (P) domain is a composite domain including a description of the anatomic segments involved; the underlying pathophysiology, whether due to reflux (R) or obstruction (O); and the etiology, whether thrombotic (T), non-thrombotic (NT), or due to a vascular malformation (congenital – C). This is exactly analogous to the E-A-P components of CEAP. For example, pelvic varices arising from bilateral gonadal reflux would be designated PBGV,R,NT (bilateral gonadal vein reflux, non-thrombotic) while those arising from an iliac compression would be designated PLCIV,O,NT (left common iliac obstruction, non-thrombotic).
Like CEAP, the SVP classification may seem overly complex and difficult at first glance. However, more than being just a complicated series of letters and numbers, both CEAP and SVP provide a logical framework for organizing a patient’s presentation in the practitioner’s mind. What symptoms does the patient have, where are any varices giving rise to the symptoms, are the varices due to reflux or obstruction, and what anatomic segments are involved? This is how we should approach every patient with pelvic venous disorders, regardless of the notation. Just as with CEAP, it does take a commitment to learning the classification and using it in daily practice.
