Technical Tips for Pelvic Venography

John White, MD
Co-Chair, AVF PeVD Summit
Complete pelvic venography remains the gold standard for the evaluation of patients with pelvic venous disease.1,2 The goals of pelvic venography in women suspected of having pelvic venous disease are to determine both the presence of anatomic abnormalities and abnormal venous flow patterns, which consist of non-cephalad flow, flow through smaller collaterals rather than large veins, and stasis within large pelvic varicosities. These anatomic and physiological derangements are best identified by pelvic venography that gently opacifies the blood without altering flow characteristics and permits visualization of gravity-enhanced direction of flow.
To accomplish this, we perform pelvic venography in the reverse Trendelenburg position and use only hand injection of contrast. We place the patient in the supine position on the x-ray table and prep and drape the right groin. The right common femoral vein is cannulated using ultrasound guidance and a 6F sheath is placed. Once this is done, the patient is placed in 20 degrees of reverse Trendelenburg position to promote the effect of gravity on venous flow(Figure 1). We begin in the left renal vein, which is cannulated with a Cobra or similarly shaped catheter. The left renal vein from the renal pelvis to the junction with the inferior vena cava must be visualized. Contrast injections in all target veins are performed by hand rather than by power injector. If there is a suggestion of renal vein compression, IVUS is performed for confirmation. Pull-out pressures are not measured since these may be normal if there is rapid reflux down the left ovarian vein. Once the left renal vein has been completely imaged, the ovarian vein is cannulated and imaged in similar fashion. If reflux is present, it is followed into the pelvis with additional injections used to determine the flow patterns within the pelvis.
The same approach is used for the left iliac venous system. The external iliac vein is injected and contrast followed into the IVC. If there is the suggestion of compression by flow diversion into smaller collateral veins, IVUS is used to assess the left common iliac vein (Figure 2). The internal iliac vein is cannulated and injected separately and the pelvic flow patterns noted. The study is completed by separately imaging the right renal, ovarian, and iliac veins. We determine the clinical significance of compression of the left renal or iliac vein by the demonstration of compression of the vein by 70% and the diversion of venous flow into smaller collateral veins.
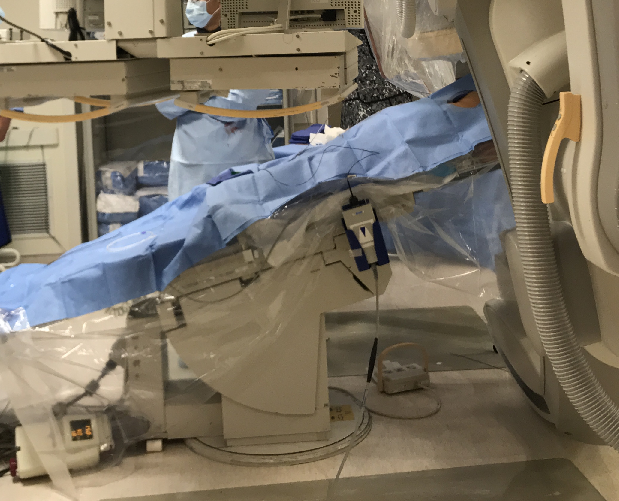
Figure 1
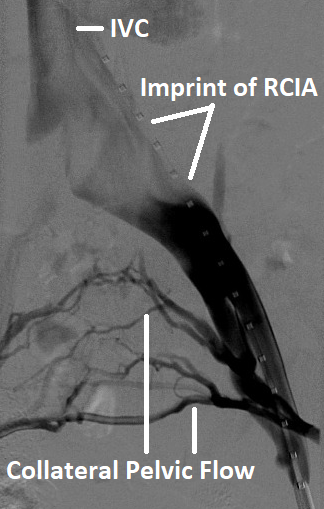
Figure 2
Figure Legends:
Figure 1: Reverse Trendelenburg position for performance of pelvic venography.
Figure 2: Lef iliac vein compression with flow diversion into smaller cross pelvic collaterals.
References
- Riding DM, Pond EJ, McCollum C, Caress AL. Seeking consensus amongst UK-based interventional radiologists on the imaging diagnosis of pelvic vein incompetence in women with chronic pelvic pain: A modified Delphi study. Phlebology. 2019 Aug;34(7):486-495.
- Shahat M, Abdelbaqy OMA, AbdelHakam AM, Ali SH, Attalla K. Can cross-sectional imaging replace diagnostic venography in pelvic venous disorder (PeVD)? J Vasc Surg Venous Lymphat Disord. 2024 Mar;12(2):101724
Open Surgical Options for Iliac Vein Compression in an Endovascular Age

Khanjan H. Nagarsheth, MD, MBA, FACS
Professor of Surgery University of Maryland School of Medicine
Endovascular stenting has become the default treatment for iliac vein compression, particularly in patients with May-Thurner syndrome. It is effective and widely adopted. Still, there are situations where an open surgical approach deserves serious consideration.
Iliac vein compression is fundamentally an anatomic problem.1 The left common iliac vein is compressed by the right common iliac artery against the spine, leading to impaired venous outflow. Over time, this can result in venous hypertension, collateral formation, and symptoms such as leg swelling, pelvic pain, and even venous ulceration.2 Stents address the narrowing, but they do not remove the source of compression.
Open reconstruction takes a different approach by addressing the anatomy directly. One technique that has shown encouraging results is anteriorization of the left common iliac vein (Figure 1). Through a transabdominal exposure, the vein is mobilized, divided, and brought anterior to the artery using a short interposition conduit. This relieves the compression entirely. In the reported series, patients experienced significant improvement in symptoms and quality of life, with durable mid-term patency.
Bypass procedures remain another option, particularly in more complex cases or after failed endovascular therapy. These include ilio-femoral-to-caval or femoral-to-femoral reconstructions. While effective, they often require adjuncts such as arteriovenous fistulas to maintain flow and are associated with a higher need for reintervention.
The key is patient selection. Open surgery is most appealing in younger patients, those with severe symptoms, or those with a long life expectancy where the durability of a stent is uncertain. It is also particularly relevant in patients with metal hypersensitivity. Nickel allergy is on the rise, and given the high nickel content in most venous stents, this can influence treatment decisions.
Stenting remains the mainstay of treatment,3 but it should not be the only option considered. Open techniques provide a durable solution that addresses the underlying anatomy. In the right patient, they can offer meaningful and lasting relief.
- May R, Thurner J. The cause of the predominantly sinistral occurrence
of thrombosis of the pelvic veins. Angiology. 1957;8:419e427
- Dunlap E, Fitzpatrick S, Nagarsheth K. Back pain and right leg
swelling: unusual presentations of May-Thurner syndrome. Cureus.
2023;15:e35984.
- Jayaraj A, Buck W, Knight A, Johns B, Raju S. Impact of degree of
stenosis in May-Thurner syndrome on iliac vein stenting. J Vasc Surg
Venous Lymphat Disord. 2019;7:195e202.
Figure 1: Left common iliac vein aneriorization
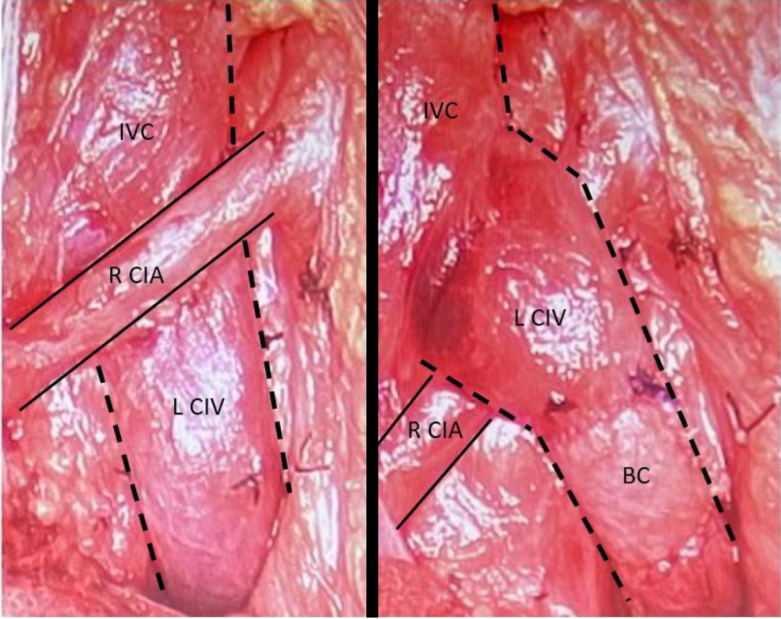
Figure 1. Pre- and post-operative left common iliac vein (LIV) anteriorization (solid lines indicate arteries; and dotted lines veins). BC, Bovine conduit; CIA, common iliac artery; CIV, common iliac vein; IVC, inferior vena cava;
L, left; R, right.
Deep Vein/Pelvic Scientific Session at AVF2026: Emerging Insights
Misaki Kiguchi, MD
Past Chair, AVF Program Committee
The Deep Vein/Pelvic session, moderated by Dr Steven Abramowitz, Professor Stephen Black, and Dr Misaki Kiguchi, highlighted the continued evolution of deep venous and pelvic interventions. Presentations focused on refining patient selection, advancing device technology, improving durability of current treatments, and better understanding mechanisms of treatment failure.
A recurring theme throughout the session was the importance of classification systems to guide clinical decision-making and determine which patients may truly benefit from intervention. Dr Houman Jalaie discussed the prognostic value of a classification system for iliofemoral stenting in patients with venous obstruction, emphasizing scenarios in which intervention may not be appropriate. Similarly, Dr Khanjan Nagarsheth introduced the Symptoms–Varices–Pathophysiology (SVP) classification for left renal vein compression disorders, proposing a structured framework for diagnosing patients with Nutcracker syndrome. Dr Steven Abramowitz also presented a propensity score–matched comparison of patients with isolated femoropopliteal deep vein thrombosis treated with either mechanical thrombectomy or anticoagulation, revisiting the ongoing debate regarding the role of infrainguinal DVT intervention.
Device performance and long-term durability also emerged as key topics. Dr Mikayla Lowenkamp presented encouraging 2-year outcomes of the VenoValve® in patients with advanced deep venous reflux. Dr Abramowitz further emphasized the importance of optimizing both inflow and outflow when performing venous stenting and reviewed the expanding mechanical thrombectomy toolkit. Dr Anusha Jacob compared deployment accuracy between nitinol and Elgiloy venous stents, highlighting important considerations in device selection. Complementing these findings, Trevin Eggleston examined endothelial coverage of venous stents over time, offering insight into device integration, while Dr Oscar Moreno described a novel in vivo model for evaluating venoplasty balloon technologies.
Pelvic venous disorders also received significant attention. Dr Peter Pappas’ group reviewed the long-term effectiveness of endovenous interventions for pelvic venous disease, while Viren Sehgal presented a thought-provoking perspective on patients’ varying presentation with May–Thurner syndrome.
Additional innovations included Dr Alperen Yıldırım’s discussion of perfusion index as a simple, objective method for monitoring patients after deep venous stenting. The presentations concluded with Professor Manj Gohel’s comprehensive overview of the mechanisms underlying venous stent failure and practical strategies to avoid them.
The session closed with a lively discussion reflecting the field’s ongoing debates—particularly around diagnosis, patient selection, treatment strategies, and long-term surveillance of patients with deep venous disease.
It was a collaborative and informative session, with contributions from speakers of all specialties, geographies, and levels of expertise.



Tips for Coil Occlusion of the Ovarian Vein

Patrick Muck, MD
Treasurer, The American Venous Forum Chair, AVF Continuing Education Committee Member, AVF Development Committee
Coil embolization can be an effective treatment for women suffering from chronic pelvic pain due to ovarian vein reflux into pelvic varicosities.1 The interruption of retrograde flow into the pelvic veins is associated with a high likelihood of relief in appropriately selected patients. While closure of the ovarian vein can be done open or laparoscopically, the endovascular placement of coils is generally considered the optimal approach.1 When the ovarian vein is dilated and the valve widely incompetent, the treatment has a high technical success rate.2
The standard technique for coil occlusion of the ovarian vein is to pack coils into the vein to create a mechanical obstruction as an adherent thrombus is generated to completely obliterate the venous lumen. This can be accomplished with a variety of materials. Initially, stainless steel was the metal used to create the devices and, subsequently, platinum was used. The stainless steel and early platinum embolization material was rather stiff.
Unfortunately, these stiff strands were capable of damaging the vein wall and eroding it over time, allowing the metal to contact other abdominal structures–most commonly the colon and the ureter. The coils then become the source of pain.3,4 In some women, the pain from the coil contacting other abdominal organs became so bothersome that excision of the ovarian vein with the coils was required for treatment. Excision generally requires laparoscopic or robotic excision of the entire length of ovarian vein that contains coils and repairing any damage to abdominal structures perforated by the coils.4
More recently, a new generation of softer platinum coils has been developed, which makes erosion of the vein wall less likely despite coil packing. Our preference has been to use the Penumbra softer platinum coils (Ruby® POD XL or Packing Coil XL coil) for endovascular occlusion of the ovarian vein. The coil is easily placed, packed so that the vein determines the shape of the coil rather than the coil forcing the vein to alter its shape to accommodate the stiff device. The “liquid metal” technology allows the coils to conform to the vein over a broad range of diameters. An 0.035” system, it is compatible with most sheaths and guidewires. It has been an effective method of venous occlusion in the setting of pelvic venous disease.
References
- Emad El Din M, Soliman M, El Kiran Y, Regal S, Youssef H, Elwakeel H, Soliman R. Ovarian vein surgical ablation versus endovascular technique for treatment of pelvic vein incompetence. J Vasc Surg Venous Lymphat Disord. 2023 Jul;11(4):801-808. doi: 10.1016/j.jvsv.2022.10.018. Epub 2023 Mar 30. PMID: 37003463; PMCID: PMC12433823.
- Wang Y, Li F, Niu G, et al. Evaluation of the feasibility, safety, and preliminary effectiveness of coil and foam embolization in patients with venous-origin chronic pelvic pain. Front Med (Lausanne). 2026 Jan 22;13:1741818. doi: 10.3389/fmed.2026.1741818. PMID: 41658582; PMCID: PMC12872915.
- Hamoodi I, Hawthorn R, Moss JG. Can ovarian vein embolization cause more harm than good? J Obstet Gynaecol Res. 2015 Dec;41(12):1995-7. doi: 10.1111/jog.12805. Epub 2015 Sep 14. PMID: 26370930.
- Medvediev M, Spesyvtsev D, Pokrovenko D, Medvedieva N, Pampukha P, Tinelli A. Laparoscopic excision of a coil-loaded ovarian vein for refractory pelvic pain after embolization: A case report. Int J Gynaecol Obstet. 2026 Feb 19. doi: 10.1002/ijgo.70902. Epub ahead of print. PMID: 41714743.
EMBOLIZE Trial Update: Advancing High Quality Evidence in Pelvic Venous Disease

Gloria Salazar, MD
Co-Principal Investigator, EMBOLIZE Trial Member, AVF Annual Program Committee and Venous CommUNITY Committee
Pelvic venous disease (PeVD), also known as pelvic congestion syndrome, is a common, yet under‑researched, cause of chronic pelvic pain which significantly impacts quality of life. Treatment decisions for these patients are often limited by variable evidence, practice variability, and insurance‑coverage hurdles. The EMBOLIZE Trial aims to address these gaps by rigorously evaluating embolization outcomes through a randomized, controlled, multicenter design—representing a major advancement in evidence‑based venous care for women with venous‑origin chronic pelvic pain.
Trial Design at a Glance
EMBOLIZE compares pelvic vein embolization versus venography alone in women with venous‑origin chronic pelvic pain due to ovarian vein insufficiency. Patients are blinded at the time of the procedure to reduce bias. Carefully selected participants are evaluated using validated patient‑reported outcome measures, including pain severity and quality of life, with a primary endpoint of change in visual analog scale (VAS) pain score at 6 months. Key inclusion and exclusion criteria reduce confounding and enhance the reliability and applicability of results.
Current Status and Call to Action
As of spring 2026, e3 academic centers—Weill Cornell Medicine, University of North Carolina Hospitals, and Northwell Health—are actively enrolling participants, with more than 80 patients pre-screened. Enrollment is currently at 17%. While stringent criteria limit enrollment, they ensure a representative population and high‑quality evidence needed to guide clinical practice and coverage decisions.
Who May Qualify
- Premenopausal women with chronic pelvic pain of venous origin (>6 months), primarily S2 patients
- Pelvic varices >5 mm and ovarian vein diameter >6 mm
- No prior pelvic venous interventions or venous stenting
Why Refer
Participants receive study‑funded procedural care and structured follow‑up. Control‑arm patients will cross over to embolization after 6 months–funded by the study. Referrals will accelerate enrollment and support the generation of high‑quality evidence for women with pelvic venous disease.
The EMBOLIZE Trial is an investigator‑initiated study sponsored by the SIR Foundation with support from Penumbra, Inc. and the VIVA Foundation.
For more information, click here or scan the QR code below:

Co-Principal Investigators and Study Contacts:
- Ronald Winokur, MD at [email protected]
- Neil Khilnani, MD at [email protected]
- Gloria Salazar, MD at [email protected]

