
Venous Thromboembolism and IVC Filter Session at AVF 2026

Arjun Jayaraj, MD
Chair, Education Council

Paola Ortiz, MD
AVF 2026 Speaker

Julianne Stoughton, MD
Past Chair, Program Committee
The Venous Thromboembolism (VTE) and Inferior Vena Cava (IVC) Filter session at the AVF 2026 highlighted emerging advances in risk prediction, basic science mechanisms of venous fibrosis, evolving clinical management of thrombosis, and contemporary patterns in IVC filter utilization.
The session opened with a presentation by Brajesh K. Lal, MD (University of Maryland) demonstrating how artificial intelligence–based predictive models can improve bleeding risk stratification in hospitalized patients being considered for pharmacologic VTE prophylaxis. The study illustrated the potential of machine learning approaches to refine individualized prophylaxis decisions beyond traditional clinical scoring systems.
Two translational science presentations by Benedict Turner, MBChB (AutoMedica) explored mechanisms underlying venous fibrosis following thrombosis. Transcriptomic analysis in murine models identified signaling pathways associated with post-thrombotic fibrosis, while a companion study demonstrated that systemic dexamethasone attenuated venous fibrosis, suggesting possible therapeutic targets to mitigate long-term complications such as post-thrombotic syndrome.
Several presentations focused on contemporary clinical management of VTE. Suchit Chidurala, MD (UT Health San Antonio) discussed evolving treatment strategies for upper extremity deep vein thrombosis, while Bartosz J. Kończyk, MD (Medical University of Silesia) presented prospective data evaluating Caprini score–based risk stratification for VTE prophylaxis in vascular surgery patients. Multiple studies examined the utilization and outcomes of IVC filters. Jonathan R. Krebs, MD (University of Florida) reported trends in filter placement and retrieval within the Vascular Quality Initiative registry, while Matthew Pergamo, MD (Stony Brook University) highlighted disparities in filter insertion and retrieval patterns. Additionally, Mohyee Ayouty, MD (Cedars-Sinai Medical Center) evaluated the role of prophylactic IVC filters in high-risk oncologic patients undergoing abdominopelvic surgery.
The session concluded with invited talks addressing ongoing challenges in VTE management. Eri Fukaya, MD, PhD (Stanford University) reviewed considerations in hypercoagulable testing following VTE, and Gaurav Parmar, MD, MPH (Massachusetts General Hospital/Harvard Medical School) discussed persistent gaps in anticoagulation therapy. Together, these presentations underscored the continued evolution of VTE care—from molecular insights into thrombosis-related fibrosis to data-driven risk stratification and ongoing efforts to optimize anticoagulation and device use.

The AVF Upper Extremity DVT Guideline: A Practical Playbook for a Growing, Under-standardized Problem

Rafael Demarchi Malgor, MD, MBA
On behalf of the AVF Guidelines Oversight Committee
Upper extremity deep venous thrombosis (UEDVT) is increasingly common in modern vascular practice, yet it remains one of the most under-standardized venous conditions we treat. The clinical scenarios are diverse: effort thrombosis in otherwise healthy patients, thrombosis around central venous catheters and cardiac devices, and malignancy-associated events that occur in a highly prothrombotic milieu. Too often, management has been extrapolated from lower extremity DVT, even though the drivers, diagnostic limitations, and procedural decisions are meaningfully different.
I had the privilege of leading the American Venous Forum (AVF) guideline effort to bring clarity to this space. The goal was not to impose rigidity, but to provide a practical playbook that improves consistency, supports shared decision-making, and helps clinicians recognize when UEDVT is “routine” and when it is a signal to look deeper, particularly for venous thoracic outlet syndrome (vTOS), catheter-related thrombosis, or cancer-associated thrombosis.
Why UEDVT needs its own guideline
UEDVT may represent a minority of all DVT events, but it generates disproportionate variation in evaluation and treatment. In practice, the uncertainties are predictable: when a negative duplex ultrasound is enough (and when it is not), how to use clinical probability and D-dimer, when to consider thrombus removal strategies, and how to manage access devices that may be both a culprit and a necessity. A guideline tailored to UEDVT allows teams to standardize the “default” approach while preserving flexibility for the high-stakes exceptions.
The organizing principle: classify by etiology
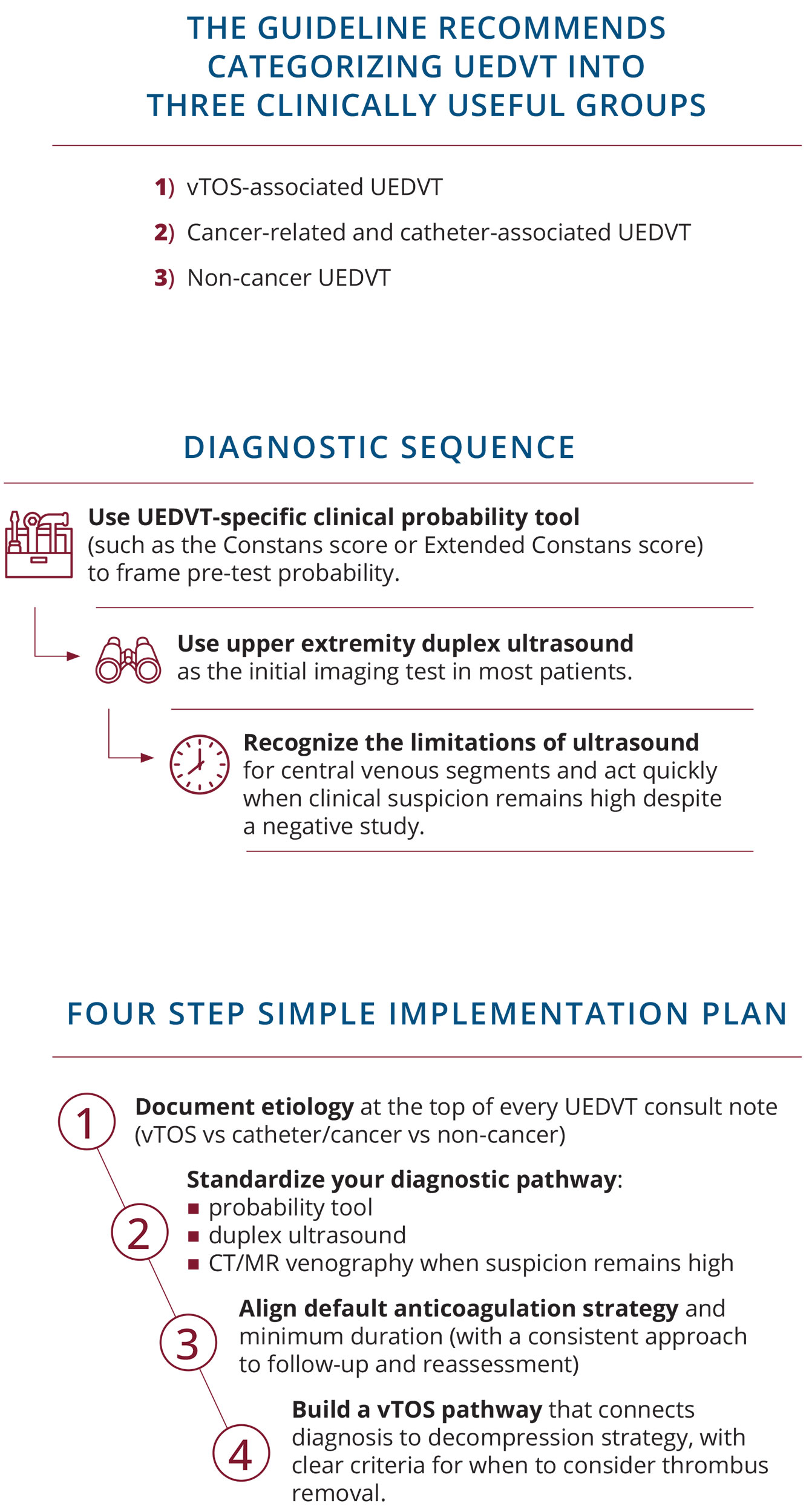
A central feature of the AVF guideline is its emphasis on etiology-based classification. Unlike lower extremity DVT, there is no widely accepted proximal-versus-distal framework in the upper extremity that reliably informs treatment. Etiology, however, directly determines what comes next. The guideline recommends categorizing UEDVT into three clinically useful groups: (1) vTOS-associated UEDVT, (2) cancer-related and catheter-associated UEDVT, and (3) non-cancer UEDVT. This shift helps clinicians align diagnostic workup, procedural considerations, and duration of therapy with the true underlying disease process.
For example, the management priorities in a young patient with effort thrombosis and suspected vTOS are fundamentally different from the priorities in a patient with an indwelling catheter who requires ongoing infusions. A shared etiologic language is the foundation for shared care pathways, and more comparable outcomes reporting across institutions.
Diagnosis: probability first, duplex first, and escalation when needed
The guideline encourages a disciplined diagnostic sequence rather than reflexive testing. First, use a UEDVT-specific clinical probability tool (such as the Constans score or Extended Constans score) to frame pre-test probability. Second, use upper extremity duplex ultrasound as the initial imaging test in most patients. Third, and this is critical, recognize the limitations of ultrasound for central venous segments and act quickly when clinical suspicion remains high despite a negative study.
When the duplex ultrasound is negative but symptoms, risk factors, or exam findings remain compelling, the guideline supports advanced imaging (CT venography or MR venography) to avoid diagnostic delay. In parallel, D-dimer should be applied thoughtfully, with particular caution in settings where it is least reliable, such as catheter-associated and cancer-associated presentations. The practical message is simple: let probability guide testing, and do not allow a negative duplex to prematurely close the case when the story does not fit.
Prevention: risk-based decisions, not automatic prophylaxis
UEDVT prevention is often shaped by habit, particularly around long-term central venous catheters. The guideline reinforces that prophylaxis is not a blanket default and should be individualized based on thrombotic risk and bleeding risk. This approach supports more rational prevention strategies, avoids unnecessary anticoagulation, and encourages clinicians to focus on patient-specific risk profiles rather than device presence alone.
Importantly, prevention discussions should also include access planning and catheter necessity. Reducing catheter dwell time and limiting line use when feasible remain practical, high-impact steps that complement any pharmacologic strategy.
Treatment: a consistent baseline with selective escalation
For most patients, anticoagulation remains the cornerstone of UEDVT treatment. The guideline supports direct oral anticoagulants (particularly oral factor Xa inhibitors) as preferred options over vitamin K antagonists for many patients with acceptable bleeding risk, with a minimum treatment duration of three months in typical scenarios. Consistence here matters: when teams align on a modern anticoagulation default, they reduce unnecessary variation and make follow-up safer and clearer.
The guideline also highlights the importance of evaluating the “unprovoked” patient. The first episode of apparently unprovoked UEDVT should trigger consideration of underlying risk factors, including malignancy and hypercoagulable states, and should prompt clinicians to confirm that a subtle mechanical driver (such as vTOS) has not been missed.
When to consider thrombus removal
Invasive thrombus removal strategies should not be routine, but they can be appropriate in carefully selected cases. The guideline supports considering early thrombus removal for acute, extensive UEDVT (generally within 21 days of symptom onset) in severely symptomatic patients with reasonable life expectancy, particularly when the goal is to reduce long-term morbidity such as post-thrombotic syndrome. The key is selection: match the intensity of therapy to the severity of symptoms, extent of thrombosis, timing, and patient-centered goals.
vTOS-associated UEDVT: treat the clot and the cause
For vTOS-associated UEDVT, the guideline emphasizes addressing the anatomic driver. When imaging and the clinical scenario support vTOS, first rib resection is recommended as the initial operative management. This reflects a core principle: durable outcomes require decompression, not anticoagulation alone. A standardized pathway that links diagnosis, symptom severity, thrombus management (when appropriate), and decompression timing can dramatically reduce fragmentation of care for these patients.
Catheter- and cancer-associated UEDVT: align care with the access plan
In catheter-associated UEDVT, anticoagulation is recommended, with catheter removal when the device is no longer needed or when alternative access is feasible. However, the guideline recognizes that catheters and ports are often essential for ongoing therapy; when removal is not feasible, treatment should proceed with a clear plan for access management and follow-up.
In cancer-associated UEDVT, clinicians must balance thrombosis control with bleeding risk and the realities of chemotherapy, procedures, and fluctuating platelet counts. A structured approach helps oncology, vascular medicine, and interventional teams coordinate decisions rather than working in parallel.
Filters: a rare tool for rare situations
Superior vena cava (SVC) filters should be reserved for highly selected patients, those with an absolute contraindication to anticoagulation and a high risk of life-threatening pulmonary embolism. The guideline’s restrained stance reflects the limited indications and the potential complications associated with these devices. In most cases, anticoagulation and careful access management remain the safer, more durable strategy.
What to implement Monday morning
Guidelines are designed to be usable. A simple implementation plan can start with four steps:
- Document etiology at the top of every UEDVT consult note (vTOS vs catheter/cancer vs non-cancer).
- Standardize your diagnostic pathway: probability tool, duplex ultrasound, and escalation to CT/MR venography when suspicion remains high.
- Align default anticoagulation strategy and minimum duration (with a consistent approach to follow-up and reassessment).
- Build a vTOS pathway that connects diagnosis to decompression strategy, with clear criteria for when to consider thrombus removal.
When these steps are standardized, teams reduce cognitive load, communicate more clearly across services, and create a reproducible foundation for quality improvement and future research.
Closing an important clinical gap
Upper extremity DVT has increased in prevalence, clinical complexity, and relevance to modern practice, yet it has long lacked standardized, evidence‑based guidance. These guidelines invite clinicians to ponder a persistent clinical gap while reducing unwarranted variation through an etiology‑driven, evidence‑based framework.
Guidelines matter when they change what clinicians do the next time they are on call. The AVF UEDVT guideline provides a shared playbook for a condition that has grown in prevalence, complexity, and importance, yet has remained under-standardized for too long. The intent is to elevate practice through clarity: classify by cause, diagnose deliberately, treat consistently, and escalate invasively only when the patient and evidence support it.
I encourage physicians and providers across all specialties caring for patients with venous disease to engage with the guideline and incorporate its framework into local pathways. Standardization is not the end of clinical judgment, it is the beginning of better, more research opportunities and consistent patient care.
Advancing Care in Pelvic Venous Disease: Join AVF in Chicago this June
Arjun Jayaraj, MD
Co-Chair, PeVD Summit Planning Committee

John White, MD
Co-Chair, PeVD Summit Planning Committee
The American Venous Forum (AVF) will host the Pelvic Venous Disease (PeVD) Summit on June 26–27, 2026 in Chicago, offering a highly specialized educational experience dedicated to one of the most complex and under-recognized areas in venous medicine.
Pelvic venous disorders remain a diagnostic and therapeutic challenge for many clinicians, often requiring a high degree of suspicion and coordination across specialties. As awareness grows, so does the need for advanced, practical education that supports accurate diagnosis and effective treatment. The PeVD Summit is designed to meet this need—equipping clinicians with the knowledge and tools necessary to improve care for this patient population.
Through case-based discussions, expert-led sessions, and real-world clinical insights, the program will explore contemporary approaches to diagnosis, imaging, and intervention. Attendees will gain a clearer understanding of disease presentation and treatment pathways, grounded in evidence-based practice and informed by leaders in the field.
A hallmark of the Summit is its multidisciplinary faculty, which includes experts in gynecology, interventional radiology, vascular surgery & physical medicine and rehabilitation. This collaborative approach reflects the reality of pelvic venous disease management, where integrated perspectives are essential to achieving optimal outcomes.
In addition to the educational program, the Summit provides an opportunity for meaningful engagement with peers and faculty who are shaping the future of venous care. The exchange of ideas and shared clinical experiences will further strengthen the collective effort to advance the field.
As the understanding of pelvic venous disorders continues to evolve, the AVF PeVD Summit stands as an important forum for education, collaboration, and progress. Clinicians from across disciplines are encouraged to participate in this unique event and contribute to improving care for patients affected by these complex conditions.

Past President Spotlight: Joseph Caprini, MD, MS, FACS, RVT, DFSVS

Parker Ball, MD
AVF Communications Intern
Dr Joseph Caprini joined the American Venous Forum in 1991, drawn by his longstanding interest in “coagulation, thrombosis, and venous disease including venous surgery.” At the time, he recalls, arterial surgeons dominated the field, but AVF offered something different. “The AVF with their group of very highly skilled vascular surgeons who were now dedicated to venous disease instead of just arterial disease… that was a perfect marriage.”
Caprini’s journey into risk assessment began unexpectedly during his military service, performing tonsillectomies on children. “Because all their tests were normal… I never operated on somebody and had a bad bleed,” he said. That early experience led to more hospital-based research, where he became known for treating bleeding disorders. “So everybody who had any kind of a bleeding problem in the hospital called on me.” It was this foundation that would eventually lead to one of the most widely used surgical tools in the world. “Probably it’s the Caprini Score… It’s the number one surgical risk assessment tool in the world, on all five continents,” he said. “Not only was there a group of people in the beginning that were so very important to its development, but… we’ve taken all of that information in and revised it in 2010 and 2013… because we’re listening to the world community and their actual experience using it.”
Early feedback wasn’t always supportive. “In 2008… CHEST recommended against the Caprini Score,” he said. But he kept going. “Don’t be discouraged and impatient when your ideas don’t pan out. Keep working on them… it takes 10 or 20 years… because new things are unfamiliar… people like to have security and consistency.” Throughout, Caprini says AVF stood apart. “That was the fellowship of the American Venous Forum,” he said, recalling a moment when Eugene Strandness left him a napkin with discussion questions before a presentation. “That was a very loving and caring thing to do.” Mentors like Eugene Strandness and Robert Rutherford made a lasting impact: “The whole rest of my career, I made sure that I followed the precepts of Robert Rutherford and Eugene Strandness.”
Now in his 80s, Caprini still rides more than 40 miles on his bike and posts monthly videos to the Venous Resource Center. “We have very little time. Don’t waste any of that time not pursuing helping others.” As for his legacy, he put it simply: “Take everything I’ve done and take it to the next level.”
“Never treat a stranger. Never kill a friend.”

New AVF Members: January/February 2026
| Name | Country |
|---|---|
| Jiyong Ahn, MD | United States |
| Samer Alaiti, MD, MSL, RVT, RPVI | United States |
| James Albert, MD | United States |
| James Andersen, MD | United States |
| Zewditu Asfaw, MD | United States |
| Candace Barber, NP | United States |
| Heather Barnhart, PT, PhD | United States |
| Joseph Bell, MD | United States |
| David Bradshaw, MSN | United States |
| Cheryl Brunelle, PT, MS, CCS, CLT | United States |
| James Chalk, MD, FACS | United States |
| Surya Challa, MD | United States |
| Eric Chuang, MD | United States |
| Kirsten Coyne, MSN | United States |
| Romina Crosby, MD | United States |
| Mary Emily Cummings, MD | United States |
| Thomas Cunningham, MD | United States |
| Shaidah Deghan Manshadi, MD, MSc | United States |
| Carlos Figueroa, PhD | United States |
| Theresa Giannini, BSN, MN, ANP-BC | United States |
| Todd Greer, MD | United States |
| Richard Grisoli, MD | United States |
| Ramona Gupta, MD | United States |
| Clint Hayes, MD, FACS, RVT | United States |
| Andrew Hearn, MD, RVT | United States |
| Nikole Hemish, PA-C | United States |
| Karl Hubach, MD, FACPh, RVT, RPhS | United States |
| Romeo Jacques, MD | Canada |
| Suzanne Jones, MD | United States |
| Tanner Jones, MD | United States |
| Jessica Jordan, NP | United States |
| Randall Juleff, MD | United States |
| Anand Kathardekar, BA | United States |
| Stephanie Katzer, CRNP, DNP | United States |
| Jasprabh Kaur, MD | United States |
| Sydney Lancer, PA-C | United States |
| Jason Le, MD | United States |
| Hali Li, PhD | China |
| Kathleen Lind, ANP | United States |
| Sarah Lucas, MD | United States |
| Astrid Marquez, NP | United States |
| Lindy McHutchison, MD | United States |
| Matthew Menard, MD | United States |
| Hyerim Nam, BS | United States |
| Kari Newell, RVT, RPhs | United States |
| Barry Oswalt, MD | United States |
| Hannah Porter, MD, MBA, MS | United States |
| Ramachandran RAVICHANDRAN, MD, FACP, RPhS, ABVLM | United States |
| Sharath Reniguntala, MD | United States |
| Amna Riaz Khan, MBBS, MRCS Ed, FCPS Gen Surgery, FCPS Vascular Surgery | Pakistan |
| David Rosen, MD, RPhS | United States |
| Kimberly Scherer, DO | United States |
| Jenna Sellers, DNP, CRNP | United States |
| Prabh Singh, MD | United States |
| Margaret Spartz, MD, MPH | United States |
| Riki Sumiyoshi, MD | Japan |
| Lucy Sun, MD | United States |
| Thomas Tamlyn, MD | United States |
| Lukas Torres, PA – C | United States |
| Irfan Ullah, MD, MPH | United States |
| Saatvik Vaishnav, MD | United States |
| Victor Viteri Perez, MD | Ecuador |
| Le Xiao, PhD | China |
| Robert Zadalis, MD | United States |
| Dennis Zagrodnik, MD | United States |
