Pelvic Congestion Syndrome: A Vascular Disorder Still Seeking Acceptance

Patrick D. Conroy, MD
Division of Vascular and Endovascular Surgery, Cooper University Hospital. Camden, NJ
Pelvic Congestion Syndrome (PCS) continues to occupy a gray zone in venous pathology:-recognized by some, questioned by others, and treated inconsistently across institutions. While PCS has been described for decades, consensus on its diagnosis and management remains elusive, in part due to symptom overlap with gynecologic and musculoskeletal conditions and a lack of standardized imaging or treatment pathways.
At our institution, a retrospective review of imaging reports from 2015–2023 identified 487 patients with CT scans and 108 patients with ultrasound reports suggesting PCS. Yet, only about 10% of these patients were referred for vascular surgery consultation. Just 29 patients ultimately underwent ovarian vein embolization. These numbers highlight a significant disconnect between imaging findings and clinical action (Figure 1). Recent discussions with OBGYN colleagues–who are the primary receivers of these radiology reports–indicate that they interpret these results as “obscure” and “incidental.” I liken this to when we as Vascular Surgeons are forwarded ABI and CT reports of Peripheral Arterial Disease when the patient exhibits no symptoms.
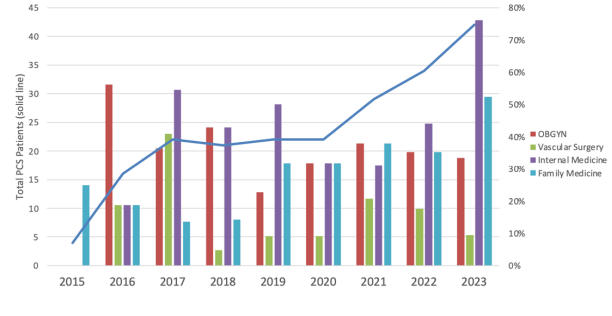
To better understand how this diagnosis is being managed, we analyzed consulting patterns in patients who had hospital diagnoses of PCS over the same time period. OBGYN, Internal Medicine, Family Medicine, and Vascular Surgery each contributed variably to PCS diagnosed patients, but no single specialty emerged as a dominant driver. Despite this, total PCS diagnoses at our institution rose steadily over the past decade, with a notable increase after 2020, yet Vascular Surgery remains consulted in only 10-23% of patients (Figure 2). This trend may reflect increased awareness, better imaging techniques, or simply greater comfort with documenting PCS as a potential cause of chronic pelvic pain.
Our findings parallel national trends. A recent abstract presented at VENOUS2025 (Feb 2025, Atlanta, GA) found that PCS diagnoses in hospitalized patients across the US. have increased substantially–nearly 3-fold– over the past 15 years (1). These data also suggest that PCS is gaining broader recognition as a legitimate vascular condition, not just at our institution but nationwide.
All of this underscores the current controversy: Is PCS underdiagnosed and undertreated? The absence of universally accepted diagnostic criteria across specialties, validated multidisciplinary symptom scores, or evidence-based referral pathways makes this a difficult question to answer. PCS exists in the borderlands of gynecology, vascular surgery, and interventional radiology– each with different philosophies, approaches, and thresholds for intervention.
Until prospective, multicenter data help establish who benefits from treatment, PCS will remain a diagnosis shaped more by belief and bias than by evidence. But the rising number of patients flagged on imaging and the widening circle of referring providers suggest that PCS is not going away. This presents a timely opportunity for collaborative research, diagnostic standardization, and multidisciplinary pathways to bring clarity to this often-dismissed venous disorder.
Reference
- Conroy P, Lombardi J, Allen S, et al. The national acceptance of pelvic congestion syndrome, a stigmatized vascular disease. J Vasc Surg Venous Lymph Dis. 2025; 13 (2): 102-136.
Figure 1. Experience with pelvic congestion syndrome diagnoses and treatment.
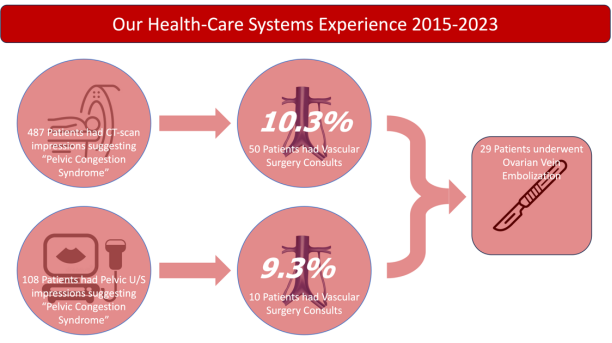
Figure 2. Vascular surgery consults for PCS trend 2015-2023.

Controversies in Abdominal-Pelvic Vein Disease – Ovarian Vein Thrombosis

Karem C. Harth, MD, MHS
Medical Director HHVI Center for Comprehensive Venous Care
Ovarian vein thrombosis (OVT) is a rare form of venous thromboembolism (VTE) for which no guidelines on management are available. Most of the OVT literature includes case studies and retrospective reviews with overall low-level evidence. The lack of strong evidence contributes to controversies surrounding its management.
Epidemiology
OVT is noted among postpartum women with an incidence between 0.05 and 0.18% following vaginal deliveries and 1 to2% following caesarean sections (1). Other at-risk groups include patients with pelvic malignancy, pelvic inflammatory disease, inflammatory bowel disease, those having pelvic surgery, hypercoagulable state, and trauma (2). Among cancer patients, rates can be as high as 37% (3). Despite their identification, there is no consensus on screening or thrombosis prophylaxis guidelines. Among screening studies of postpartum women, rates can be as high as 30% with MRI, but remain of unclear significance.
Diagnosis
Clinically symptomatic OVT can be nonspecific and challenging to diagnose. Prolonged fever that is unresponsive to antibiotics, and pelvic, abdominal, or flank pain in the postpartum patient are most common (1). Asymptomatic patients are identified while undergoing imaging for malignancy or during a post-operative state. Iatrogenic cases require thrombophilia work-up to guide care. Imaging modalities include computed tomography (CT) scan, ultrasound (US), and magnetic resonance imaging (MRI). CT is widely available, has good sensitivity (SN 77-100%) and specificity (SP 62.5-99%), but involves radiation (1-3). MRI has good SN (92-100%) and SP (100%); it is less available and more costly. US is highly operator-dependent and has overall low SN (50-56%) and SP (41-99%) (3). A standardized diagnostic algorithm for first-line imaging is lacking and is reflected in the literature by a heterogeneity of reports.
Management
Antibiotics: In symptomatic postpartum patients with fevers and abdominal pain, antibiotics are the mainstay; but their role is unclear in the patient without systemic signs of infection.
Anticoagulation: Type and duration of anticoagulation are variably recommended across the literature, with no guidelines for the various groups at risk. In some reports, evaluating asymptomatic patients with incidental OVT following debulking pelvic surgery, no anticoagulation was prescribed (3,4). No one anticoagulant is recommended uniformly and most cases appear to respond well to LMWH or DOAC’s. Certainly, LMWH remains the best treatment option among pregnant women or those who are breastfeeding. Duration is variably reported, but generally involves a treatment of 3-6 months, with potentially longer in idiopathic or malignancy cases (2).
While overall rates appear low, a missed diagnosis of OVT is not insignificant. VTE extension into the iliac veins, PE, IVC, or left renal vein was noted among 6-10% of patients (3). PE rate among postpartum women can be as high as 25% in some reports. Other complications can be recurrent VTE and major bleeding, at 8 and 2% respectively (3). Recurrent events occurred between 3 mos to 6 yrs from initial diagnosis in the following: lower extremities, PE, contralateral OVT, IVC extension, renal vein, and portal vein thrombosis. It is unclear how this relates to initial anticoagulation choice or duration. Death was primarily noted in the setting of cancer or sepsis. OVT should be considered in the above-mentioned at-risk groups and should be treated with anticoagulation with duration determined by the clinical scenario.
References
- Labropoulos N, Malgor R, Comito M, Gasparis A, Pappas P, Tassiopoulos A. The natural history and treatment outcomes of symptomatic ovarian vein thrombosis. J Vasc Surg: Venous and Lymphatic Disorders. 2015;3:42-47.
- Christy J, Jarugula D, Kesari K, Kunadi A. Idiopathic bilateral ovarian vein thrombosis. BMJ Case Rep 2021; 14:e238243
- Monnet M, Dufrost V, Wahl D, Morel O, Agopiantz M, Zuily S. Epidemiology, natural history, diagnosis, and management of ovarian vein thrombosis: a scoping review. J Thromb Haemost. 2024;22:2991-3003
- Yassa NA, Ryst E. Ovarian vein thrombosis: a common incidental finding in patients who have undergone total abdominal hysterectomy and bilateral salpingo-oophorectomy with retroperitoneal lymph node dissection. Am J Roentgenol. 1999;172:45–7.
You are invited to the Japanese Society of Phlebology Annual Meeting!
The JSP Annual meeting is a significant event that brings together experts from various fields, and we are excited about the upcoming meeting. We have also organized a short trip for attendees to explore the local area. Learn more below!


Treatment of Pelvic Venous Disorders: What first?

Arjun Jayaraj, MD
Vascular Surgery; The Rane Center
Pelvic venous disorders (PeVD) have become the subject of increasing interest from the medical community. Despite this, a clear pathway for the management of these conditions has remained elusive. For example, in symptomatic patients with combined gonadal vein reflux and iliac vein compression, what should be treated first and why? Many such combinations can arise since the disorder encompasses left renal vein compression, gonadal vein reflux, iliac vein compression, internal iliac vein reflux, and superficial venous reflux, reflecting both obstruction and reflux. This brings us to the Symptoms-Varices-Pathophysiology (SVP) classification and its utility. The classification uses a combination of clinical and pathophysiological features across 4 zones (Figure 1) to characterize an individual’s PeVD. However, often patients have symptoms across multiple zones, challenging the development of a management plan. This is why the history and physical exam (H&P) are so important in the management of PeVD. Careful consideration must be given to the nature of symptoms and their effect on the patient’s quality of life. That information informs the determination of the most impairing symptom (MIS). The focus of treatment in multizone PeVD should be on the MIS, with a clear understanding by the patient that a stepwise treatment approach may be required, and the expected relief may not necessarily occur with the first intervention. Eg, if a patient has left flank pain, hematuria, and pelvic venous pain, but the flank pain is the most impairing, then comprehensive diagnostic work must be carried out to evaluate the status of the left renal vein, the gonadal veins, the iliac veins including the internal iliac vein, and pelvic venous reservoir with treatment focused on correction of any left renal vein compression that has been diagnosed. If, after this, the pelvic venous pain is still bothersome, then that can be managed by focusing on residual culprit pathophysiology. At times, the dilemma can be particularly challenging. An example is. a patient presenting with pelvic pain and dysmenorrhea with gonadal vein reflux, left common iliac vein compression, and internal iliac venous reflux. Here, the symptoms are restricted to a single zone (zone 2) and MIS is not helpful. One way to approach this is to determine the problem that has the most significant hemodynamic impact (MSHI). Given that the hemodynamic impact of a compressed common iliac vein on venous hypertension in the pelvic reservoir is likely to be the most significant, correction of such obstruction is expected to lead to greater symptom relief than abolition of a refluxing gonadal vein. Often, correction of the obstruction in the CIV leads to correction of retrograde flow in the internal iliac vein and symptom amelioration. On the other hand, if despite this, the patient continues to be symptomatic, then correction of the gonadal vein reflux or abolition of internal iliac vein reflux is in order, with the sequence again determined by the hemodynamic contribution of each problem. These issues serve to highlight the complexities involved in the management of patients with PeVD, the importance of a thorough H&P, comprehensive diagnostic assessment, and treatment targeted toward mitigation/resolution of the MIS/MSHI and addressing any residual problems as needed and in sequence.
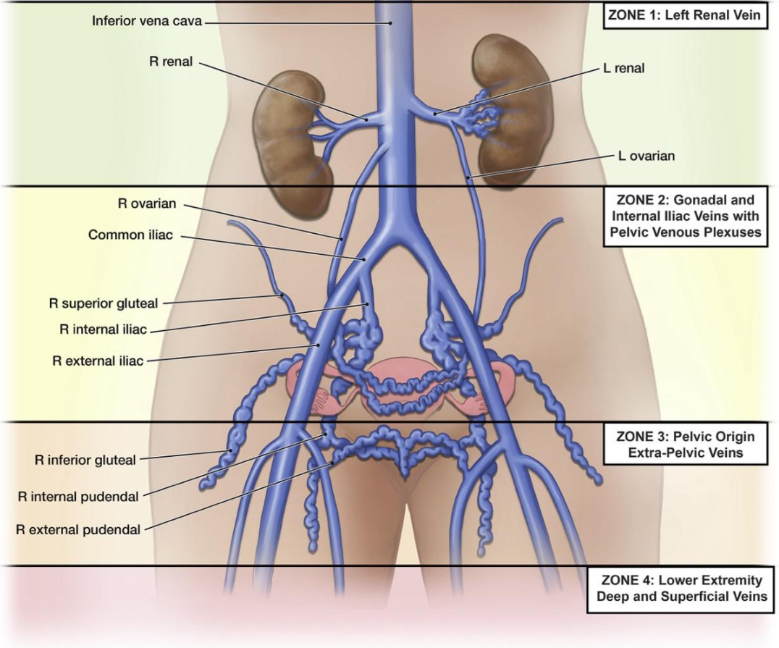
Fig 1. Anatomic zones of pelvic venous disorders. From Meissner MH, Khilnani NM, Labropoulos N, et al. The Symptoms-Varices-Pathophysiology classification of pelvic venous disorders: A report of the American Vein & Lymphatic Society International Working Group on Pelvic Venous Disorders. J Vasc Surg Venous Lymphat Disord. 2021 May;9(3):568-584.