Vein Specialist
2025May/June
Table of contents
Editor’s Message
Steve Elias, MD
Controversies in Pelvic-Abdominal Venous Disease
Nutcracker: A Tough Nut to Crack
Kathleen Ozsvath, MD, FACS
The Symptoms-Varices-Pathophysiology Classification of Pelvic Venous Disorders
Mona Li, MD
Pelvic Congestion Syndrome: A Vascular Disorder Still Seeking Acceptance
Patrick D. Conroy, MD
Controversies in Abdominal-Pelvic Vein Disease – Ovarian Vein Thrombosis
Karem C. Harth, MD, MHS
Treatment of Pelvic Venous Disorders: What first?
Arjun Jayaraj, MD
EMBOLIZE Trial: Advancing Treatment for Chronic Pelvic Pain
- Neil Khilnani, MD
- Gloria Salazar, MD
- Ronald Winokur, MD
AVF News
A Message from the AVF President
Joseph Raffetto, MD
Leadership Corner: Ruth L. Bush, MD’s Presidential Address
Jillian Norbut
Join us at the Vein & Lymphatic Summit on July 18-19, 2025
- Peter Gloviczki, MD, PhD
- Monika Gloviczki, MD, PhD
Submit an abstract for AVF 2026
Misaki Kiguchi, MD
AVF’s Advocacy Focused on Translating Evidence into Policy and Fair Reimbursement
Harry Ma, MD, PhD
EDITOR-IN-CHIEF
Steve Elias, MD
EXECUTIVE EDITOR
John Forbes, MBA
MANAGING EDITOR
Allison DeGroff
COVER ARTIST
Christine Rataj
PUBLICATION DESIGNER
Anthony Eaves
Editor’s Message

Steve Elias, MD
Editor-In-Chief
Vein Specialist
A Brief Summer Story
I was a lifeguard for 7 years–early to mid-70’s;high school and college; Nassau County, Long Island, NY; 1 year on the ocean and 6 years at the pools. At the start of every season we’d get our gear: sweatshirts, sweatpants, T-shirts, and a few bathing suits–skimpy Speedo briefs. No one thought that this was not quite appropriate. It was de rigueur for male lifeguards in the 70’s. All summer we would walk around in 3 ounces of stretch nylon in front of the public. The young female guards were issued a rather modest one-piece suit. Who thought this was a good look? Then the look changed. Now male guards wear shorts and female guards can don bikinis.
But in 2025, the skimpy brief is back. Not for lifeguards, but for the public, the male public. The tables have turned. It seems that they are wanted– or rather fashion designers think that they should be wanted this summer. Todd Snyder, a menswear designer whom I had never heard of, introduced his Mykonos brief this year. Three solid colors and an inside pocket for keys or whatever else one deems important to put inside a tiny suit. It’s relatively inexpensive at $95. Other fashion houses are offering pricier options: Burberry’s $440; Gucci $800; and Miu Miu $950. They all look like $48 Speedos to me. I should have kept my suits and sold them today as vintage.
In Vein Specialist we haven’t saved anything from the past to sell you now. Rather, this issue brings you new thoughts about pelvic and abdominal vein disease. The articles aren’t skimpy and we don’t charge you anything for them. Our contributors address controversies and give you something to think about when you see patients with pelvic vein problems. Topics include: renal vein compression, ovarian vein thrombosis, SVP classification, who to treat and how to treat, and why is pelvic congestion still not accepted as a real entity. We also have AVF news about leadership, the upcoming Vein & Lymphatic Summit, abstract submission information, and our new members’ roster. Our society needs new leaders and new ideas to move forward.
The men’s fashion world has also moved forward this summer with the spare, sparse, skimpy swimsuit. Apparently, they are for every size and shape. Miu Miu is offering 7 colors in 14 different sizes. I guess I didn’t realize there are 14 different sizes for men. Time will tell where this trend goes. Speedo is reaping benefits since they are the industry standard. Apparently, more people are wearing Speedos. And more people are treating vein disease whether they wear Speedos or not. Our job at Vein Specialist is to bring you the latest trends and ideas in the vein world. We don’t care if you wear swim briefs or swim trunks or a one-piece or bikini. We just care that you understand and treat vein disease the right way. Read this issue in whatever summer swimsuits you choose. And when you swim this summer, pull those drawstrings tightly enough so the suit stays up.
Nutcracker: A Tough Nut to Crack

Kathleen Ozsvath, MD, FACS
Chief of Surgery, Samaritan Hospital, Troy, NY
Left renal vein (LRV) compression can be seen in one-half to three- quarters of CT angiograms in asymptomatic patients (Nutcracker Phenomenon, NP) (1). Nutcracker Syndrome (NS) refers to symptomatic patients, first described in 1937 (2). When the left renal vein lies anteriorly between the superior mesenteric artery and the aorta posteriorly, it is known as anterior NS (3,4). Less often, when the vein lies between the aorta and the vertebral bodies, it is known as posterior NS or pseudo NS. Radiologic studies have reported the normal aorto-mesenteric angle (AMA) to be between 38 and 68o. Pressure gradients between the LRV and IVC have been associated with an angle of less than 35o (4-7). A gradient of >3mmHg has been associated with renal venous hypertension (3). Classical presentation of symptomatic NS includes hematuria, proteinuria, and flank pain (7,8). The incidence of NS is not known. The literature describes a bi-modal peak occurring in childhood, peaking at the second decade, and the second occurring in the third/fourth decades (5.6). The highest prevalence is in females with a low body mass index (8,9). Ultrasonography, CTA, MRV can be used together to determine the presence of entrapment of the LRV; venography and intravascular ultrasound has been more recently utilized (10,11). Duplex ultrasound can record peak systolic velocities between the hilar LRV and at the compression of the aortomesenteric LRV segment. Ratios between 4.0:1 and 5.0:1 are thought to be significant. Demonstration of LRV stretching and compression seen on B mode support the diagnosis of NS. Venography with intravascular ultrasound (IVUS) can characterize and determine the presence of a pressure gradient (≥3 mm Hg) (7). Conservative management in young patients is undertaken, as three-quarters will have resolution of symptoms within 2 years (12,13). Adults with persistent symptoms should consider alternative treatment. First described by Stewart et al, transposition of the LRV has been described; however, other treatment approaches include hybrid procedures, including laparoscopic and endovascular (14-16). Re-intervention rates for LRV re-stenosis have been reported to occur in one-third to two-thirds of cases. Large gonadal veins can be transposed to decompress the LRV and kidney as well. Experienced centers have reported on laparoscopic interventions. Left kidney auto transplantation has been reported, especially in patients with re-stenosis. Endovascular stent placement has been described, but complications have been reported including stent thrombosis and migration (17,18). Erben, et al reported on 37 patients (30 women and 7 men) who were treated surgically by LRV transposition. Adjuvant treatments included vein patches, and intravascular stent. Early re-intervention rates for LRV re-stenosis were 8%; and late was 22%, with 82% (9 of 11 patients) treated with endovascular stent placement. At 24 months, primary, assisted primary, and secondary patency were 74%, 97%, and 100%, respectively. Complete resolution of symptoms occurred in 87% of patients (20). Re-intervention rates have been described in one third of patients due to re-stenosis of the transposed LRV (16). Reports using endovascular means to treat NS exist, however stent migration has been reported in 7.5% of patients (17). Wu, et al reported on 75 patients who underwent renal vein stenting. Of the 49 patients, 5 had stent migration (21). These authors recommend measuring LRV diameter during Valsalva to help with stent sizing. A case with hybrid surgical and endovascular repair has been reported with intraoperative renal vein stenting, with the stent then secured in place with Prolene™ sutures (22). The recent classification of signs and pathophysiologic symptoms of pelvic venous disease has defined renal vein obstruction based on symptoms, presences of varices, and pathophysiology. This has allowed specialists to organize the disease based on anatomic consideration (23). The treatment of Nutcracker Syndrome ranges from the classical open surgical techniques to more modern endovascular techniques and hybrid procedures. Most series and case studies are reported on low numbers of patients. Although more common in women, not enough data are available to understand gender-specific differences in treatment outcomes (24).
References
- Kim SH. Doppler US and CT diagnosis of Nutcracker Syndrome. Korean J Radiol 2019; 20:1627-37.
- Erben Y, Gloviczki P, Kalra M, et al. Treatment of nutcracker syndrome with open and endovascular interventions. J Vasc Surg Venous Lymphat Disord. 2015;3(4):389-396.
- Ananthan K., Onida S., Davies A. Nutcracker Syndrome: An update on current diagnostic criteria and management guidelines. Eur J Vasc Endovasc Surg 2017; 53:886–894.
- Yun SJ, Lee JM, Nam DH, Ryu JK, Lee SH. Discriminating renal nutcracker syndrome from asymptomatic nutcracker phenomenon using multidetector computed tomography. Abdom. Radiol. (NY) 2016; 41:1580–1588. Doi: 10.1007/s00261-016-0717-8.
- Bhanji A, Malcolm P, Karim M. Nutcracker syndrome and radiographic evaluation of loin pain and hematuria. Am. J. Kidney Dis. 2010 Jun;55(6):1142-5. doi: 10.1053/j.ajkd.2009.10.010.6. Cardarelli-Leite L, Velloni FG, Salvadori PS, Lemos MD, D’Ippolito G. Síndromes vasculares abdominais: achados de imagem característicos. Radiol Bras. 2016;49(4):257–263.
- Kolber MK, Cui Z, Chen CK, Habibollahi P, Kalva SP. Nutcracker syndrome: diagnosis and therapy. Cardiovasc Diagn Ther. 2021;11(5):1140-1149.
- Shin JI, Lee JS, Kim MJ. The prevalence, physical characteristics and diagnosis of Nutcracker syndrome. Eur J Vasc Endovasc Surg. 2006; 32:335–336.
- He Y, Wu Z, Chen S, et al. Nutcracker syndrome—How well do we know it? Urology 2014; 83:12–17. Doi: 10.1016/j.urology.2013.08.033.
- Granata A, Distefano G, Sturale A, Figuera M, Foti PV, Palmucci S, Basile A. From Nutcracker Phenomenon to Nutcracker Syndrome: A pictorial review. Diagnostics (Basel). 2021 Jan 11;11(1):101. doi: 10.3390/diagnostics11010101. PMID: 33440614; PMCID: PMC7826835.11. Poyraz AK, Firdolas F, Onur MR, Kocakoc E. Evaluation of left renal vein entrapment using multidetector computed tomography. Acta Radiol. 2013;54(2):144–148.
- Meissner MH, Khilnani NM, Labropoulos N, et al. The Symptoms-Varices-Pathophysiology classification of pelvic venous disorders: A report of the American Vein and Lymphatic Society International Working Group on Pelvic Venous Disorders. Vasc Surg Venous Lymphat Disord. 2021; 9 (3): 568-584.
- Avgerinos ED, McEnaney R, Chaer RA. Surgical and endovascular interventions for nutcracker syndrome. Semin Vasc Surg. 2013;26(4):170–177.
- Said SM, Gloviczki P, Kalra M, et al. Renal Nutcracker syndrome: surgical options. Semin Vasc Surg. 2013;26(1):35–42.
- Reed NR, Kalra M, Bower TC, Vrtiska TJ, Ricotta JJ 2nd, Gloviczki P. Left renal vein transposition for nutcracker syndrome. J Vasc Surg. 2009 Feb;49(2):386-93; discussion 393-4. doi: 10.1016/j.jvs.2008.09.051. PMID: 19216958.16. Velasquez CA, Saeyeldin A, Zafar MA, Brownstein AJ, Erben Y. A systematic review on management of nutcracker syndrome. J Vasc Surg Venous Lymphat Disord. 2018;6(2):271-278.
- De Macedo GL, dos Santos MA, Sarris AB, Gomes RZ. Diagnosis and treatment of the Nutcracker syndrome a review of the last 10 years. J Vasc Bras 2018; 17(3): 220-228.
- Wang X, Zhang Y, Li C, Zhang H. Results of endovascular treatment for patients with nutcracker syndrome. J Vasc Surg. 2012; 56:142-148.
- Fuentes-Perez A, Bush R, Kalra M, et al. Systematic review of endovascular versus laparoscopic extravascular stenting for treatment of Nutcracker syndrome. J Vasc Surg Venous Lymphat Disord. 2023; 11(2): 433-441.
- Erben Y, Gloviczki P, Kalra M, et al. The treatment of nutcracker syndrome with open and endovascular interventions. J Vasc Surg Venous Lymphat Disord. 2015; 3(4): 389-96.
- Wu Z, Zheng X, He Y, et al. Stent migration after endovascular stenting in patients with nutcracker syndrome. J Vasc Surg Venous Lymphat Disord. 2016;4(2):193-199.
- Jayaraj A, Gloviczki P, Peeran S, Canton L. Hybrid intervention for treatment of the nutcracker syndrome. J Vasc Surg Cases. 2015;17(1):268-271.
- Meissner MH, Khilnani NM, Labropoulous N, ret al. The symptoms varices pathophysiology classification of pelvic venous disorders. A report of the American Vein and Lymphatic Society International Working Group on Pelvic Venous Disorders. J Vasc Surg Venous Lymphat Disord. 2021; 9 (3): 568-584.
- Ozsvath K, Raffetto JD, Lindner E, Murphy EH. Venous compression syndromes in females: a descriptive review. Semin Vasc Surg 2023; 36 (4): 550-550.

The Symptoms-Varices-Pathophysiology (SVP) Classification of Pelvic Venous Disorders
Mona Li, MD
Assistant Professor of Surgery, Medical College of Wisconsin
The American Vein and Lymphatic Society (AVLS) convened an international multidisciplinary panel to develop a valid and reliable classification instrument for pelvic venous disorders (PeVD). Published by Meissner, et al in 2021 and analogous to the CEAP classification, the goal was to create a standardized approach to the characterization, diagnosis. and management of PeVD (1). This instrument defines the variable overlapping clinical presentations that are characteristic of PeVD. It eliminates historical syndromic nomenclature (Pelvic Congestion, May-Thurner’s, and Nutcracker Syndromes), which do not accurately depict the complex interactions among them. Note that the SVP is not designed to reflect disease severity. Similar patients with similar pathophysiology can now be grouped together. This is important to facilitate the future development of clinical trials and disease-specific outcome measures to improve treatments. Greater recognition of PeVDs as a cause for symptoms, particularly for chronic pelvic pain in women, will increase the evaluation for PeVD and decrease misdiagnosis. An individual’s classification is designated as SVPAHE.
The symptoms, signs (varices), and pathophysiological mechanisms are divided into 4 anatomic zones and are arranged in descending order from the renal veins (Figure 1):
Zone 1 are SVP associated with the left renal vein.
Zone 2 are SVP associated with the gonadal and internal iliac veins with pelvic venous plexuses.
Zone 3 are SVP associated with pelvic origin extra-pelvic veins refluxing through the pelvic escape points.
Zone 4 are SVP in the lower extremity deep and superficial veins. Zone 4 is not part of SVP and should be classified with CEAP.
The classification system begins with Symptoms designated with subscripts 0-3:
1 – renal symptoms of venous origin;
2 – chronic pelvic pain of venous origin;
3 – symptoms associated with extra-pelvic varices
and is further subdivided by location of these varices and venous claudication (a,b,c) (Figure 2).
Next, V is for varices (signs) and the subscripts for this section are divided by the location of the varicosities:
1 – varices around the renal hilum;
2 – pelvic varices;
3 – extra-pelvic varices, with separation between vulvar varices or varicoceles and the non-saphenous varices of the leg (a,b) (Figure 3).
Finally, P the pathophysiological mechanisms, is separated into 3 sub domains:
A is for anatomy – all the possible involved anatomic veins with laterality or bilaterality reported;
H is for hemodynamics – either obstruction (O) or reflux (R);
E is for etiology: T is for a thrombotic etiology causing reflux or obstruction from prior DVT, NT is non-thrombotic, where reflux is either primary, or secondary to obstruction from external compression; and finally, C which is from a congenital etiology (Figure 4, Tables IV, V, VI from the reference).
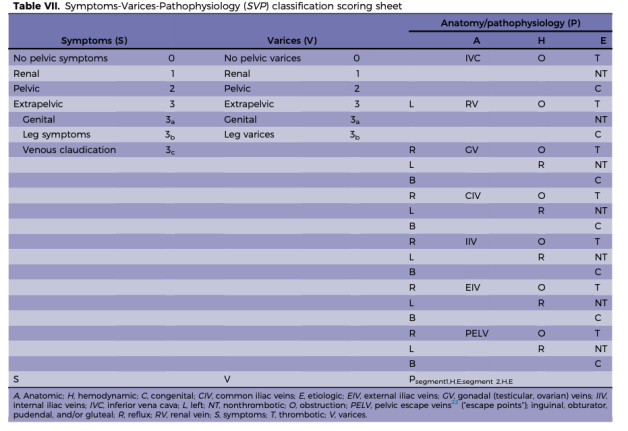
A scoring sheet to aid in using this classification scheme appears in Figure 5. For example: the classification for a patient with pelvic congestion syndrome, with chronic pelvic pain from bilateral ovarian reflux, would be: S2V2PBGV,R,NT. As another example, the classification for a patient with Nutcracker Syndrome with left flank pain and hematuria would be: S1V1PLRV, O, NT. If there are overlapping anatomic segments, they are separated with a semi-colon and the list order is from Zone 1 – Zone 3. Refer to Meissner et al., for all the details on the development and use of the SVP classification (1), which can be used in conjunction with the CEAP classification.
Reference
- Meissner MH, et al. The Symptoms-Varices-Pathophysiology classification of pelvic venous disorders: A report of the American Vein and Lymphatic Society International Working Group on Pelvic Venous Disorders. J Vasc Surg Venous Lymphat Disord. 9:568-84, 2021.
All figures are from:
Meissner, MH. et al. The Symptoms-Varices-Pathophysiology classification of pelvic venous disorders: A report of the American Vein and Lymphatic Society International Working Group on Pelvic Venous Disorders. J Vasc Surg Venous Lymphat Disord. 9:568-84, 2021
Figure 1:
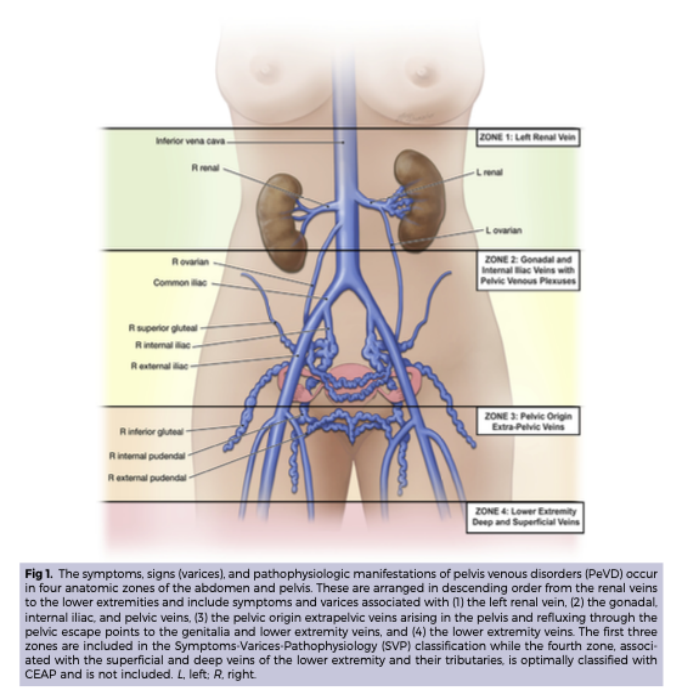
Figure 2:
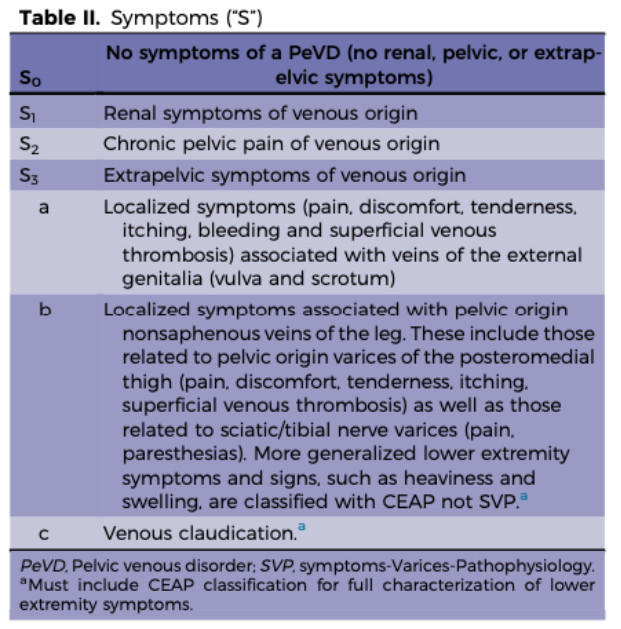
Figure 3:
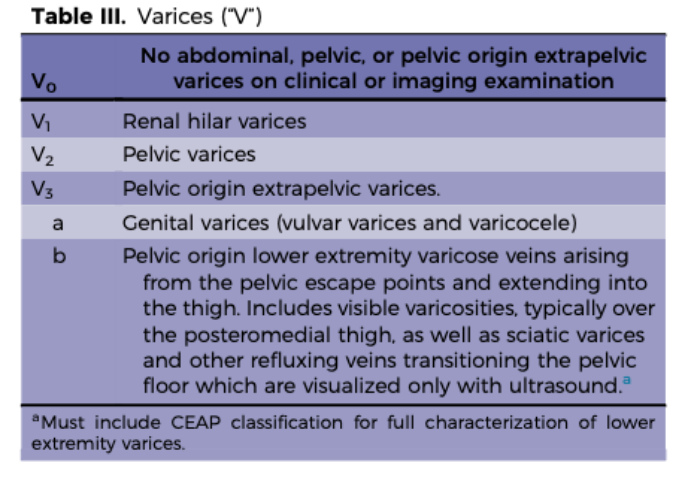
Figure 4:
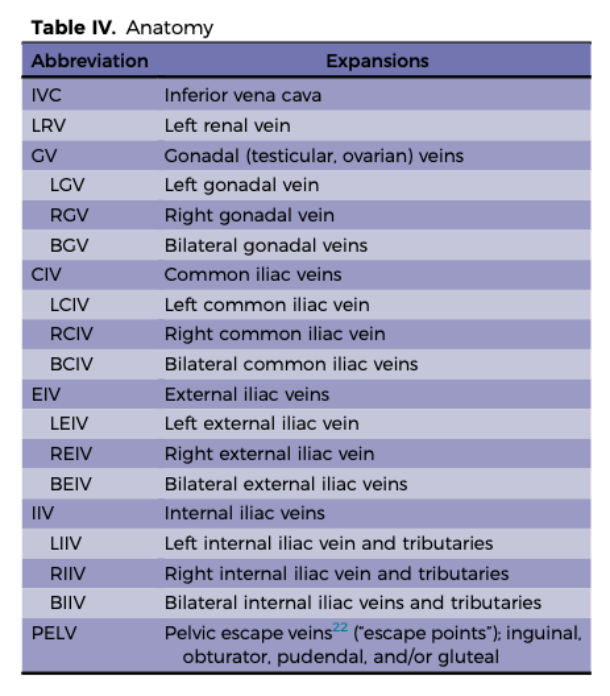
Figure 5:
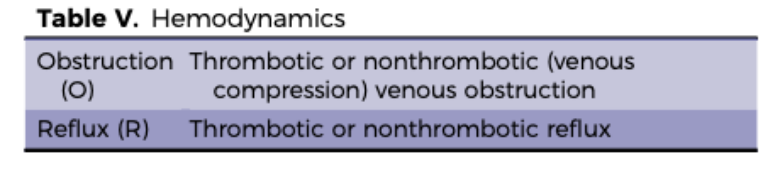
Figure 6:
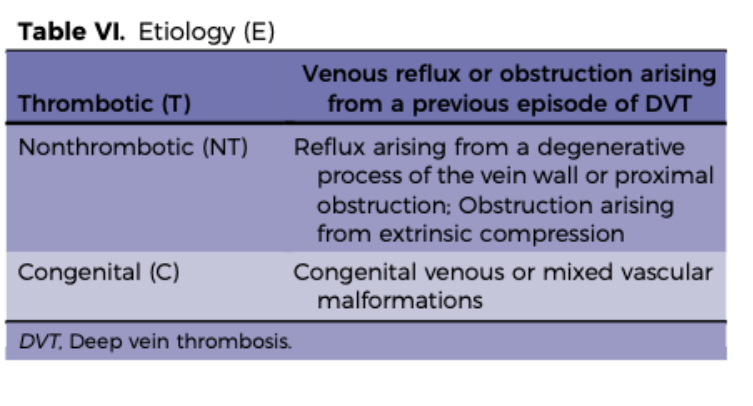
Figure 7: