Vein Specialist
2026The Great Masquerader
When Things Aren’t What They Seem
Table of contents
Editor’s Letter
Steve Elias, MD
Improved Venous Hemodynamics, Progressive Hyperpigmentation: Looking Beyond Venous Disease
Juan Carlos Jimenez, MD, MBA; Clinical Professor, UCLA Health
Mitali Doshi, MD; Vascular-Integrated Resident, UCLA Health
Schamberg Disease
Robert R. Attaran, MD; Associate Professor, Yale School of Medicine
When Reflux is not Really Reflux
Blake Iceton, MD; Vascular Medicine Consultant, Mayo Clinic
Eri Fukaya, MD; Vascular Medicine, Stanford University
When “Venous Leg Ulcers” Aren’t Really Venous
Raghu Kolluri, MD; System Chief of Vascular Medicine; OhioHealth
The Great Masquerader: When Things Aren’t What They Seem
Kush Desai, MD; Professor, Northwestern University
Unmasking the Masqueraders: When Leg Ulcers Aren’t What They Seem
Karen L Bauer DNP, CNP-FNP, FAAWC, CWS
Suzanna Fitzpatrick, DNP, CNP-ACNP, CNP-FNP, FAANP
AVF News
AVF 2026 in Denver: Elevating Education, Hands-On Learning, and Professional Connections
Misaki Kiguchi, MD; Co-chair, Program Committee
Julianne Stoughton, MD; Co-chair, Program Committee
The AVF Annual Meeting: An American Conference with an International Heart
Rashad Bishara, MD; Chair, International Committee
American Venous Forum Achieves Record Membership in 2025, Strengthening Its Global Leadership in Venous and Lymphatic Care
Pamela Kim, MD; Chair, Membership Committee
Advancing Care for Pelvic Venous Disorders
Arjun Jayaraj, MD; Co-chair, Summit Planning Committee
John White, MD; Co-chair, Summit Planning Committee
Elias Receives Sushruta Award
Rick Kennedy, PA-C, MBA; Executive Director, Lakhanpal Vein Foundation
Compression Socks versus Medical Gradient Compression: What’s the Difference?
Margie Hopkins; U.S. Clinical Marketing Manager, Essity
Past President Spotlight: Thomas Wakefield, MD
Parker Ball; AVF Communications Intern
Healing Veins, Restoring Lives: The HHPF Veins & Vascular Access Team Needs YOU!
Kay Weeden; Director, Hackett Hemwall Patterson Foundation
Fostering Stronger Bonds with the American Venous Forum
Palma Shaw, MD; President, International Society for Women Vascular Surgeons
Someone Who Knows Somebody Who Knows You
Gary Burnison; CEO, Korn Ferry
EDITOR-IN-CHIEF
Steve Elias, MD
EXECUTIVE EDITOR
John Forbes, MBA
MANAGING EDITOR
Allison DeGroff
COVER ARTIST
Christine Rataj
PUBLICATION DESIGNER
Anthony Eaves
Editor’s Letter

Steve Elias, MD
Editor-In-Chief
Vein Specialist
Special Delivery
So, the question was: yes or no? If so, how much? If not, why not? I don’t carry that much cash. Nowadays one doesn’t have much use for cash. China has been cashless for years. Pennies are gone. Maybe we need cash for tips. The parking valet, your favorite maître d’, your garbage collectors, and the mail carrier. More about the mail carrier later. It was the maître d’ that the yes or no question was about.
New Year’s Eve. Early dinner at our favorite French restaurant, La Goulue, in New York City. Go there often. Have special dinners there. Know Daoud, the maître d’, well for years. Nice guy. Does he do anything special for us? Sometimes. Not always. Not on this New Year’s Eve. He was distracted. Late night celebrations later that night. The regular crowd was there early as were we. Had a really good meal, but do I give him a “thank you for the year” tip. If so, how much? I had $31.00 in my wallet. Clearly not enough. Big dilemma. Give nothing[ give $31? My wife and I were in a quandary. Which was worse, nothing or $31? Which is less insulting. We weren’t sure. Is too little worse than nothing or is nothing worse than too little?
In Vein Specialist we give you more than nothing and certainly more than enough. We give you what you need to know and we give you what you want. This issue’s theme is “The Great Masquerader.” We’ve asked our contributors to give some examples of things that might be venous, but really are not. They have identified many non-venous problems that can seem venous at first blush. We have all been fooled. Minocycline skin changes, Schamberg’s disease, false reflux, ulcers of other causes, and a venous mass. The articles are brief and to the point and you can learn something from each one of our excellent contributors. They all worked hard on short notice. This is a must-read. We also bring you good news about our membership. We hit a record number at the end of 2025 and it will only continue to get better. Not resting on our laurels, the inaugural Pelvic Venous Disease Summit will take place this June 27 and 28 delivering needed information about this timely and complicated disease state.
And Tony our mail carrier delivers every day except Sunday. “Neither snow nor rain nor heat nor gloom of night stays these couriers from the swift completion of their rounds.” This is inscribed in the New York City post office building. The original saying is from the Greek historian Herodotus who was referring to Persian carriers who actually had an organized postal system in 500 BC. And Tony continues the tradition of delivery on foot and only on foot. Why not a mail truck? Well, Tony had some issues. Tony enjoyed distilled spirits. Tony enjoyed them during the day when delivering mail in his mail truck. When the jig was up, Tony was not fired but rather his mail truck was taken away from him. He now walks no matter what the conditions. He is in good shape and has a nice tan with some very well-defined tan lines. The perks of purgatory.
And that’s where my wife and I were on New Year’s Eve. Purgatory. We were stuck between Scylla and Charybdis. The two immortal Greek monsters located on the narrow Strait of Messina. A lot of famous Greeks needed to navigate this strait; Odysseus, Jason, Aeneas, et al. What choice they made determined their fate. We had a choice: no thank you tip or a $31 one. We chose no tip, the better of two evils. Nothing was better than something. In Vein Specialist, it is the opposite. We give you a whole lot of something and not nothing. And my wife and I will give something the next time we see Daoud. Not sure about the appropriate amount. But I’m sure ChatGPT knows and we can always ask Tony. Tony always delivers.
Improved Venous Hemodynamics, Progressive Hyperpigmentation: Looking Beyond Venous Disease

Juan Carlos Jimenez, MD, MBA
Clinical Professor,
UCLA Health

Mitali Doshi, MD
Vascular-Integrated Resident, UCLA Health
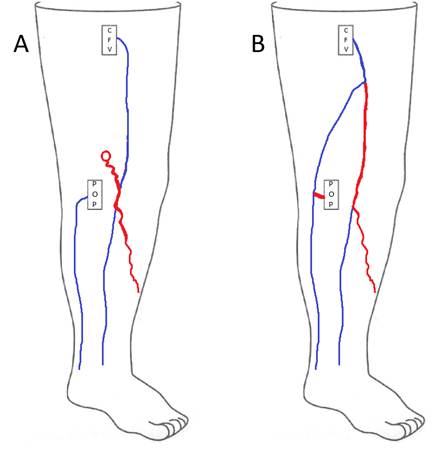
A 56-year-old male furniture designer presented with long-standing bilateral lower extremity discoloration, swelling, aching, pain, and throbbing (Figures 1A and 1B). His symptoms had been present for many years and were exacerbated by prolonged standing for several hours daily as part of his occupation. He had consistently worn graduated compression stockings without meaningful symptomatic relief.
Office-based duplex ultrasound demonstrated severe reflux of the bilateral great saphenous veins (GSVs), with dilation up to 8 mm. He subsequently underwent bilateral radiofrequency ablation of the GSVs, resulting in significant improvement in leg aching, swelling, and fatigue.
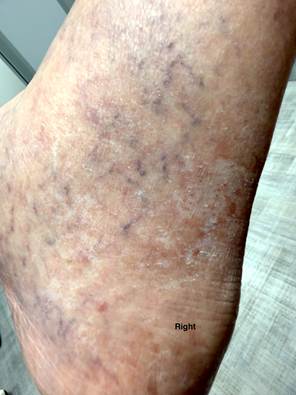
One year later, the patient returned with complaints of progressive bilateral ankle and foot discoloration (Figure 2). Repeat duplex ultrasound demonstrated occluded bilateral thigh GSVs, consistent with successful ablation. Additional findings included bilateral common femoral vein reflux, below-knee GSV reflux with small-caliber veins (approximately 2 mm), and superficial tributary vein reflux.
Before pursuing additional venous interventions, the patient was referred for outpatient dermatologic evaluation. During this consultation, he reported long-term use of oral minocycline for acne. Dermatology performed a punch biopsy, which revealed findings compatible with drug-induced hyperpigmentation. Iron and Fontana–Masson stains were both positive within the dermal pigment. No malignancy was identified. The presence of pigment staining with both iron and Fontana–Masson was noted to be consistent with drug-induced hyperpigmentation, including that associated with minocycline use. Correlation with the full clinical context was recommended.
Minocycline was discontinued, and the patient was transitioned to doxycycline due to concern for medication-related pigmentation. Following discontinuation of minocycline, the patient reported partial improvement in skin discoloration, though complete resolution did not occur. He continues to take doxycycline with persistent hyperpigmentation and has elected not to pursue further venous procedures currently.
Discussion
This case illustrates a rare and instructive presentation of chronic venous insufficiency with progressive lower extremity discoloration following successful bilateral GSV ablation, in which the predominant contributor to worsening pigmentation was ultimately identified as drug-induced hyperpigmentation rather than recurrent venous pathology. It underscores the importance of obtaining a comprehensive medication history during initial and follow-up venous evaluations and highlights how changes in venous stasis may obscure alternative etiologies of lower extremity hyperpigmentation. In this patient, a multidisciplinary approach was essential in arriving at the correct diagnosis and guiding appropriate management.
Figure Legends
Figures 1A (Left) and 1B (Right): Lower leg hyperpigmentation prior to great saphenous vein ablation.


Figure 2: Worsening bilateral lower leg hyperpigmentation one year after great saphenous vein ablation. The patient continues on doxycycline for chronic acne.

Schamberg Disease

Robert R. Attaran, MD
Associate Professor, Yale School of Medicine
Seeing venous disease referrals, sooner or later, you will come across a patient with pigmented areas on the legs, suspicious for venous insufficiency. On further questioning, you will learn that the patient does not have any of the typical signs and symptoms of chronic venous insufficiency. No heaviness or aching. The pigmented areas can disappear and reappear. Though they tend to occur in the legs, they are not exclusive to the gaiter zone. In fact, they can occur over the trunk.
Schamberg disease has several pathologic descriptors, such as progressive purpuric (pigmented) dermatosis. Considered benign, it is a form of lymphocytic capillaritis, associated with fragile capillaries, red blood cell extravasation, and subsequent hemosiderin deposition, which can mimic the stigmata of venous disease. The precise cause is unknown, but genetics may play a role. Case reports have indicated a potential association with certain medications.
Medical therapy is chiefly for cosmetic purposes and can include topical steroids, pentoxifylline, and light therapy.
Patients with suspected Schamberg disease are typically referred to a dermatologist. In the absence of other symptoms, venous imaging is not warranted.
Photo from website of pcds.org.uk

Photo from Acad Derm Nevada

When Reflux is not Really Reflux

J. Blake Iceton, MD
Vascular Medicine Consultant,
Mayo Clinic
Eri Fukaya, MD
Vascular Medicine,
Stanford University
Case: 35F presented with painful right posteromedial thigh and knee vein, concerned for thrombosis given history of DVT in both parents. However, duplex ultrasound was unremarkable with no clots or reflux, and the patient was treated conservatively with compression stockings. She returned 6 years later noting leg fatigue worse at the end of nursing shifts. A repeat duplex performed 6 months earlier showed axial reflux in the right great saphenous and small saphenous veins (Figure 1).
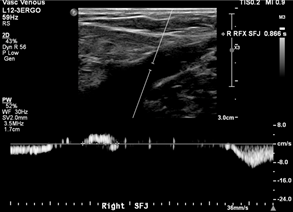
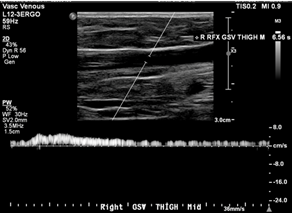
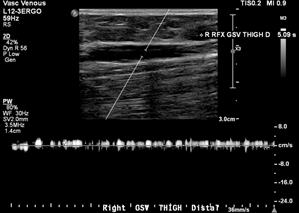
Images showed questionable reflux and it was revealed that the study was performed in a moderate reverse Trendelenburg (RT) position. There was mild reflux at the SFJ in response to Valsalva and a long duration reflux in the thigh and leg in response to distal augmentation with the signal becoming intermittent distally.
Is this real venous reflux?
Investigation: A low amplitude reflux could cause this pattern with gaps in reflux representing amplitude dipping below the detectable or filtered threshold. However, this could also represent a failure of RT position to generate sufficient downward pressure to achieve complete valve closure, which can result in a valve fluttering effect as blood passes through. We repeated the duplex ultrasound with the patient standing, and this was negative for reflux in any GSV segment.
Discussion: Optimal assessment of venous reflux with duplex imaging requires upright positioning. Tthis serves as a reminder that supine and even RT positioning can cause false positive results in addition to false negatives. Steep RT can provide accurate results and ease the ergonomic burden on technologists, but any questionable results should be double-checked in the standing position.
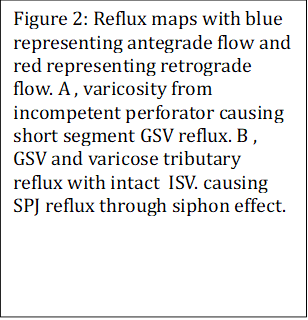
Other occurrences where reflux is misdiagnosed result from anatomical variance or incomplete mapping. Common femoral vein reflux is often only measured superior to the SFJ, but there is no proximal valve in nearly 1 in 3 people. Reflux identified here in the absence of distal deep reflux or SFJ incompetence should not be reported as significant deep reflux. Likewise, segments of superficial veins can demonstrate reflux where a tributary joins and leaves in between valves. This is seen with varicosities arising primarily from incompetent perforators (Figure 2A). A rarer phenomenon is a siphon effect created from a vessel loop, such as in anterograde diastolic flow of the intersaphenous vein (formerly Giacomini vein). Here, outward flow in the SPJ is not pathologic but rather a hemodynamic response to reflux proximally in the leg (Figure 2B). These findings highlight that complete mapping of the lower extremity venous system with careful consideration of sources is necessary to ensure appropriate diagnosis of patients.
When “Venous Leg Ulcers” Aren’t Really Venous

Raghu Kolluri, MD
System Chief of Vascular Medicine,
Ohio Health
Most clinicians who treat venous disease see leg ulcers every week, and the default assumption is often chronic venous insufficiency because venous leg ulcers (VLUs) are the most common type. However, not every ankle ulcer is venous and several important mimics can look deceptively similar, at least initially. Making the diagnosis early is best, as most of these patients endure significant morbidity before seeking professional help. At the very least, if ulcers fail to respond to good compression, appropriate wound care, and correction of venous reflux, it’s time to step back and reconsider the diagnosis.
The variable presentation of VLUs and the extensive differential diagnosis have been described in a recent article (1). Following are 3 such masqueraders: the etiology of the first 2 cases is driven by microvascular thrombosis rather than venous hypertension; and a third, often overlooked entity, hydroxyurea-associated leg ulceration, is a medication-related complication that vein specialists should recognize.
Case 1:
A 42-year-old woman with rheumatoid arthritis presents with recurrent, intensely painful ankle ulcers that partially heal and then recur despite consistent compression therapy and prior vein treatments. A venous insufficiency study demonstrated great saphenous vein reflux from the proximal to mid-calf. The small saphenous vein was ablated. Examination revealed small, shallow ulcers with surrounding ivory-white stellate scars and mottled hyperpigmentation from previously healed ulcers.

Diagnosis: Livedoid vasculopathy
How it differs from venous ulcers: Pain and recurrence are the most important clues. Livedoid vasculopathy is characterized by severe pain out of proportion to ulcer size and by atrophie blanche (porcelain-white scars left by healed ulcers) lesions, which are typically small, shallow, and recurrent, often accompanied by livedo reticularis. Venous disease may coexist, which can obscure the diagnosis but does not explain the ulcer pattern.
Management pearls: Livedoid vasculopathy is a thrombotic microangiopathy, not a vasculitis. Anticoagulation is the cornerstone of treatment, with growing evidence supporting DOACs or low–molecular-weight heparin. Evaluation for thrombophilia and autoimmune disease is appropriate. Compression may help symptoms but is rarely sufficient on its own.
Case 2:
A 55-year-old woman with a history of unprovoked deep vein thrombosis and a history of TIApresented with a painful, nonhealing distal pretibial ulcer that progressed to the current stage in 3 weeks. The lesion had irregular, violaceous borders with areas of necrosis and worsened despite compression therapy.

Diagnosis: Antiphospholipid antibody–associated ulcer
How it differs from venous ulcers: APS-related ulcers result from arterial and microvascular thrombosis rather than venous reflux. They are often painful, ischemic-appearing, and may have purpuric or necrotic features. A history of unexplained thrombosis (venous or arterial), pregnancy loss in women, or livedo reticularis should raise suspicion.
Management pearls: Systemic anticoagulation is essential. In high-risk APS, warfarin remains standard therapy. Local wound care alone is ineffective unless the underlying hypercoagulable state is treated.
Case 3:
A middle-aged man with essential thrombocythemia on long-term hydroxyurea presented with chronic bilateral lower-extremity edema and a history of painful, recurrent blistering lesions around the posterior aspects of both ankles and the Achilles regions. The lesions healed, but recurred intermittently despite compliance with 20-30 mm Hg compression socks.

Diagnosis: Hydroxyurea-associated leg ulcers
How it differs from venous ulcers: Hydroxyurea-associated ulcers can occur in the peri-malleolar area, but are disproportionately painful, often bilateral, and occur in atypical locations – the posterior ankle area, Achilles region, or dorsum of the foot rather than the medial malleolus. Lesions may begin as blistering erosions and persist or recur despite appropriate compression.
Management pearls: Ulcers often fail to heal unless hydroxyurea is discontinued. Early coordination with hematology is critical.
Take-home message:
Leg ulcers with disproportionate pain, atypical location, unusual morphology, or failure to respond to venous therapy are unlikely to be VLUs and should prompt a broader differential.
REFERENCE
- Kolluri R, Fukaya E, Krishna S, Dean S. Venous leg ulcers: A review of clinical variability and differential diagnosis. Vasc Med. 2025 Apr;30(2):218-237.

