Vein Specialist
2025July/August

Table of contents
Editor’s Letter
Steve Elias MD
Industrial Innovation
A Living Network Meta-Analysis: Understanding Varithena’s Role in Chronic Venous Disease
Boston Scientific
In Service of Patient and Provider: Mobilizing Technology with Methapharm
Methapharm
Sigvaris Motion Flow Tech®
Sigvaris
Revolutionizing Relief: The AWCS Compression System’s Impact on Chronic Venous Insufficiency Management
Sun Scientific
The Pounce™ Venous Thrombectomy System: Dual-action Removal of Fresh or Organized Clot
Surmodics
AVF News
Advance Your Expertise: Attend the 2025 Venous Early Career Course
Robert Attaran, MD; Chair, AVF Early Career Committee
VLS 2025 Recap: Advancing Venous & Lymphatic Care in Every Setting
Allison DeGroff; AVF Director of Strategic Initiatives
Fueling Innovation in Venous and Lymphatic Disease: The American Venous Forum’s Research Grants
Eri Fukaya, MD; Chair, AVF Research Committee
Board Member Spotlight: Misaki Kiguchi, MD
Jillian Norbut; AVF Communications Intern
Past President Spotlight: Mark Meissner, MD
Parker Ball; AVF Communications Intern
Pioneering Vascular Surgery in Space: Onboard Wound-care During Long-duration Human Deep Space Exploration
Dora Babocs, MD; Baylor College of Medicine, Postdoctoral Research Fellow
Putting Leadership on the Map
Gary Burnison; Chief Executive Officer, Korn Ferry
CMS’s Proposed 2026 Physician Fee Schedule will help office-based specialists
Harry Ma, MD, PhD; Chair, AVF Health Policy Committee
AVF 2026: Join us in the heart of the Mile High City!
Misaki Kiguchi, MD; Co-Chair, AVF Program Committee
Julianne Stoughton, MD; Co-Chair, AVF Program Committee
EDITOR-IN-CHIEF
Steve Elias, MD
EXECUTIVE EDITOR
John Forbes, MBA
MANAGING EDITOR
Allison DeGroff
COVER ARTIST
Christine Rataj
PUBLICATION DESIGNER
Anthony Eaves
Spoiled Necessity or Necessarily Spoiled?

Steve Elias, MD
Editor-In-Chief
Vein Specialist
F. Scott Fitzgerald is purported to have said to Ernest Hemingway, “The rich are different from you and me.” Hemingway’s response, “Yes, they have more money.” Hemingway, while being an intellectually inciteful person, may have missed the mark. Was F. Scott speaking strictly about money? Ernest obviously thought so but what if Fitzgerald was thinking more broadly about so many other things: lifestyle, attitude, morals, etc? People are not defined solely by their monetary worth. Perhaps Hemingway was thinking narrowly and only from his point of view.
The Tote Taxi Service has a narrow purpose: bring your stuff (almost any stuff) from NYC to the Hamptons. It’s not a moving company but more of a “what whim do you have that you want satisfied today” type of service. They recently transported 48 croissants from the L’Appartement 4F Bakery in Manhattan to East Hampton. Cost? $500 not including the cost of croissants. Why? Because it is really hard to find a good croissant in East Hampton? I don’t know; I don’t usually consume croissants. Ordered in the morning, arrived in the afternoon. Instant gratification for some hungry, wealthy soul. Fitzgerald was right; the rich are different from you and me. No judgment. Just stating the facts of the Tote Taxi Croissant Caper. You decide if it was money well spent.
In Vein Specialist we mostly spend time and not much money to give you the latest in the vein world. This issue focuses on contributions by our industry partners. We give industry a deserved voice. The articles are by 7 of them– some large and some small– but all innovative: Surmodics, Koya, Sun Scientific, Methapharm, Boston Scientific, Inari, and Sigvaris. The topics are very timely. Some insight. It is very hard to have industry contribute due to the fact that there are a lot of hurdles they need to overcome internally such as their compliance lawyers. So, we congratulate our contributors. Read their articles. And read the other non-industry articles.
In this issue we have brought you more useful information than the Tote Taxi Service ever could. At least for now. Their operation is still small. They plan on growing. Expanding to Palm Beach Florida and a Boston-to-Cape Cod route. Currently, the business is like a maquette, a small preliminary model of something that will ultimately be much larger–such as a sculptor’s model, an architect’s small-scale building. If the maquette was made by a famous person, they are worth something. Maquettes are collected by wealthy people. Maquettes by Picasso and Henry Moore have sold for millions. The rich are different from you and me. Most rich people don’t read each issue of Vein Specialist. But you do. We hope you realize each issue is a complete work, not a maquette. Read on.
A Living Network Meta-Analysis: Understanding Varithena’s Role in Chronic Venous Disease

Katie Allega
Boston Scientific, Medical Affairs Manager
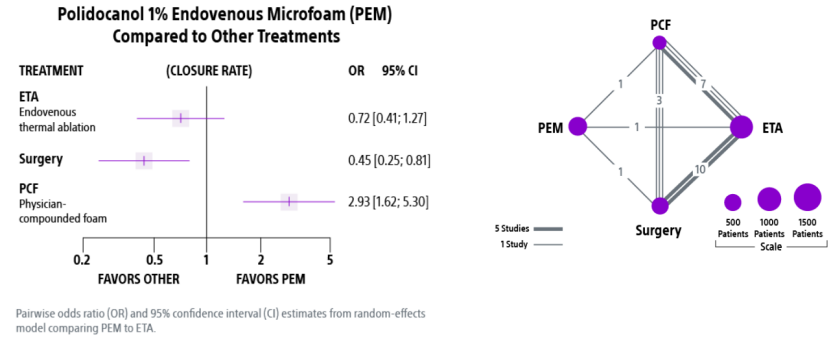
In treating patients with chronic venous insufficiency (CVI), making informed treatment decisions can be challenging due to limited direct comparisons among commonly used therapies. While VarithenaTM (polidocanol 1% endovenous microfoam), endovenous thermal ablation (ETA), and physician-compounded foam (PCF) are all widely utilized to treat superficial vein incompetence, few randomized head-to-head trials exist. To address this evidence gap, a Living Network Meta-Analysis (Living NMA) was designed to provide an evolving, comprehensive assessment of comparative literature that will be updated regularly as new data emerge.
A network meta-analysis (NMA) enables simultaneous comparison of multiple treatments, using both direct and indirect evidence from a network of both randomized controlled trials (RCTs) and comparative, non-randomized studies. The initial publication of the Living NMA was spearheaded by Lowell Kabnick, MD, and was published in Journal of Vascular Surgery: Venous and Lymphatic Disorders in April 2024 (1). This publication included 13 studies (6 RCTs and 7 comparative, non-randomized studies) comparing Varithena™ (PEM), ETA, and PCF, with outcomes focused on truncal vein closure from 3 months up to 6 years. The results showed that Varithena™ was not statistically different from ETA, but significantly outperformed PCF in achieving durable vein closure. In fact, Varithena™ had an almost 3 times increase in odds of vein closure as compared to PCF (1).
Importantly, this was never intended to be a static analysis. From the beginning, the Living NMA was structured to support quarterly updates, ensuring that clinicians have access to the most current data as the body of evidence grows. The most recent update added 7 additional trials (2 RCTs and 5 comparative, non-randomized studies), bringing the total to 20 studies. Despite the expanded dataset, the core conclusions remained consistent:
- Varithena™ and ETA showed no statistical difference in closure outcomes
- Varithena™ continues to demonstrate superior closure rates compared to PCF, sustained across all time points
These consistent findings enhance clinical confidence in Varithena’s™ performance and validate the value of an agile, living evidence model. By continuously integrating new high-quality data, the Living NMA provides a transparent, up-to-date resource to support evidence-based treatment decisions in CVI.
To review the full analysis, please visit: https://www.varithena.com/en-us-hcp/clinical-evidence/living-network-meta-analysis.html
- Kabnick LS, Jimenez JC, Coogan SM, Gache L, Frame D, Gunnarsson C, Ozsvath K. Comparative effectiveness of non-compounded polidocanol 1% endovenous microfoam (Varithena) ablation versus endovenous thermal ablation utilizing a systematic review and network meta-analysis. J Vasc Surg Venous Lymphat Disord. 2024 Nov;12(6):101896. doi: 10.1016/j.jvsv.2024.101896. Epub 2024 Apr 26. PMID: 38679141; PMCID: PMC11523335.
The DEFIANCE Study: A Pioneering Randomized Controlled Trial of Mechanical Thrombectomy Versus Anticoagulation Alone for Iliofemoral Deep Vein Thrombosis

Steven Abramowitz, MD
Vascular Surgery, MedStar Washington Hospital Center

Stephen Black, MD
Consultant Vascular Surgeon and Professor of Venous Surgery, Guy’s and St Thomas’ Hospital, Kings College London

Xhorlina Marko, MD
Senior Staff Interventional Radiologist, Henry Ford Health System and Adjunct Clinical Assistant Professor, Michigan Medicine
Patients diagnosed with iliofemoral deep vein thrombosis (DVT) are at increased risk of developing post-thrombotic syndrome (PTS), a condition associated with chronic morbidity. Although the standard of care, anticoagulation therapy alone does not actively remove thrombus, leaving patients vulnerable to PTS. (1) Intervention for acute DVT using catheter-directed thrombolysis (CDT) has shown mixed effectiveness for preventing PTS. (2-4) Moreover, lytic-based therapies have increased risks of bleeding and require patients to be monitored in the intensive care unit (ICU), increasing critical resource utilization and care costs. (5) Recent innovations to mechanical thrombectomy have improved safety and efficacy in the endovascular management of iliofemoral (DVT) and may prove to be the future of intervention.
Mechanical thrombectomy using the ClotTriever System (Inari Medical) is a catheter-based approach to remove thrombus from within the vein lumen without the need for thrombolytics. Results from the ClotTriever Outcomes (CLOUT) registry demonstrate the safety and effectiveness of this treatment through a 2-year follow-up. (6-8) Furthermore, a recent meta-analysis comparing early thrombus removal techniques identified advantages of mechanical thrombectomy over CDT, including a markedly lower risk of major bleeding and reduced ICU use. (9)
Although the available evidence for thrombectomy as a DVT treatment is promising, randomized data evaluating mechanical intervention against anticoagulation alone are needed. DEFIANCE aims to address this through a prospective international RCT investigating mechanical thrombectomy plus standard anticoagulation versus anticoagulation alone for patients with symptomatic unilateral iliofemoral DVT. (10) The primary endpoint is a hierarchical composite assessing treatment failure or escalation as adjudicated by an independent medical monitor and PTS severity at 6 months using the Villalta scale.
The importance of DEFIANCE is underscored by the recently published 2025 European Society for Vascular Medicine (ESVM) guidelines on the interventional treatment of venous thromboembolism. (11) The guidelines provide Class IIa recommendations that catheter-based therapies be considered for patients with severe symptoms secondary to acute proximal DVT and that mechanical thrombectomy be preferred over CDT. Notably, the authors recognize DEFIANCE as the only ongoing RCT specifically addressing this question,
In summary, the DEFIANCE trial marks a significant milestone in the field of venous intervention. With its robust study design, clinically relevant endpoints, and alignment with the emerging guidelines, it is well-positioned to generate definitive evidence on the role of mechanical thrombectomy in the management of iliofemoral DVT. AVF readers are encouraged to follow this pivotal study, which has the potential to reshape treatment pathways and improve outcomes.
References
- Bauer G. Nine years’ experience with heparin in acute venous thrombosis. Angiology. Apr 1950;1(2):161-9. doi:10.1177/000331975000100205
- Enden T, Haig Y, Klow NE, et al. Long-term outcome after additional catheter-directed thrombolysis versus standard treatment for acute iliofemoral deep vein thrombosis (the CaVenT study): a randomised controlled trial. Lancet. Jan 7 2012;379(9810):31-8. doi:10.1016/S0140-6736(11)61753-4
- Comerota AJ, Kearon C, Gu CS, et al. Endovascular Thrombus Removal for Acute Iliofemoral Deep Vein Thrombosis. Circulation. Feb 26 2019;139(9):1162-1173. doi:10.1161/CIRCULATIONAHA.118.037425
- Notten P, de Smet A, Tick LW, et al. CAVA (Ultrasound-Accelerated Catheter-Directed Thrombolysis on Preventing Post-Thrombotic Syndrome) Trial: Long-Term Follow-Up Results. J Am Heart Assoc. Jun 2021;10(11):e018973. doi:10.1161/JAHA.120.018973
- Misono AS, Mouawad NJ, Niekamp AS, Bunte MC. Inferring acute economic aspects of endovascular deep vein thrombosis management from a literature-based comparative cohort analysis. JVS-Vascular Insights. 2024;2doi:10.1016/j.jvsvi.2024.100117
- Dexter D, Kado H, Shaikh A, et al. Safety and Effectiveness of Mechanical Thrombectomy From the Fully Enrolled Multicenter, Prospective CLOUT Registry. Journal of the Society for Cardiovascular Angiography & Interventions. 2023/02/23/ 2023:100585. doi:10.1016/j.jscai.2023.100585
- Bisharat MB, Ichinose EJ, Veerina KK, et al. One-Year Clinical Outcomes Following Mechanical Thrombectomy for Deep Vein Thrombosis: A CLOUT Registry Analysis. J Soc Cardiovasc Angiogr Interv. Mar 2024;3(3Part A):101307. doi:10.1016/j.jscai.2024.101307
- Dexter D, CLOUT Investigators. Complete Two-Year Outcomes in Patients Receiving Mechanical Thrombectomy for Deep Vein Thrombosis in the CLOUT Registry. Presented at: Vascular InterVentional Advances. Nov 4, 2024; Las Vegas, NV.
- Turner BRH, Jasionowska S, Shea J, et al. A Systematic Review and Meta-analysis of the Efficacy and Safety of Lytic and Non-lytic Early Thrombus Removal Technologies for Iliofemoral Deep Vein Thrombosis. Ann Surg. May 27 2025;doi:10.1097/SLA.0000000000006765
- Abramowitz SD, Marko X, D’Souza D, et al. Rationale and design of the DEFIANCE study: A randomized controlled trial of mechanical thrombectomy versus anticoagulation alone for iliofemoral deep vein thrombosis. Am Heart J. Mar 2025;281:92-102. doi:10.1016/j.ahj.2024.10.016
- Schlager O, Campello E, Madaric J, et al. 2025 ESVM Guidelines on interventional treatment of venous thromboembolism. Vasa. Jun 30 2025;doi:10.1024/0301-1526/a001211
Case Study: Non-Pneumatic Compression Device for the Management of Active Venous Ulceration and Chronic Venous Disease

Heather Barnhart PT, PhD
Koya Medical, Director of Clinical Operations
An 88-year-old man diagnosed with secondary lymphedema due to chronic venous insufficiency was referred for Dayspring, non-pneumatic compression device (NPCD), to manage the secondary effects of phlebolymphedema and subsequent venous leg ulcers. Despite conservative measures for many months, the patient continued to endure significant edema, heaviness/achiness, pain, hyperplasia, recurrent cellulitis, fibrosis, hyperpigmentation, hyperkeratosis, and chronic/recurrent venous ulcerations. He used a variety of compression wraps and bandages, yet was not able to use compression stockings. NPCD was recommended to manage progressive symptoms, mitigate disease progression, and increase adherence with compression utilization.
The patient’s medical history is significant for chronic venous disease of the right extremity, chronic obstructive pulmonary disease, hypertension, Type II diabetes mellitus, insomnia, dizziness, colostomy, and total hip replacement. Current medications at treatment initiation included: diclofenac sodium, fluticasone propionate, furosemide, hydroxyzine HCL, levalbuterol chloride, rivaroxaban, and tiotropium bromide.

Right lower extremity
October 2024
Pre-Dayspring use
Dayspring was initiated in October of 2024 for the right leg for 60 minutes daily. The patient was able to ambulate during treatment to the bathroom and kitchen, reducing interference with his activities of daily living. After one month of use, the patient’s symptoms significantly improved, and after 2.5 months (10 weeks), the patient reported his wounds had resolved, swelling had reduced, and skin texture returned to normal.

January 2025
One month Dayspring Use

February 2025
2.5 months Dayspring Use
On February 17, 2025, the patient’s wife reported, “This is so comfortable, pleasant, and easy to put on. The sores went away, the elephant skin has almost all healed, and his leg has not swollen.”
