
May/June Issue of Vein Specialist
New Treatment Paradigm and Associated
Economic Impact for Managing Chronic Venous Disease via Mechanical Thrombectomy

Nicolas Mouawad, MD
McLaren Health
Michigan, MI

A. Baqai, MD
Ascension Medical Center
Illinois, IL
Post-thrombotic syndrome (PTS), a form of chronic venous disease (CVD), affects up to 50% of deep vein thrombosis (DVT) patients and is similar to cancer or congestive heart failure in its quality-of-life (QoL) implications.1,2 In its most severe cases, open venous wounds can develop secondary to residual thrombus that transform into chronic venous fibrotic obstructions (CVFOs) that impede cephalad flow, increasing venous pressure, and are classified as clinical, etiological, anatomic, and pathophysiological 6 (CEAP-6) venous disease1 (Figure 1). In the US alone, these wounds amass an annual cost of ~$32B.3,4
Current treatments for CVD are limited to anticoagulation, compression therapy, stenting, venoplasty, and surgery. For CEAP-6 patients, treatment options also include debridement, reflux ablation, and skin substitutes. These treatment strategies deliver only palliative care, and wounds could recur in 70% of patients within six months.4 As a result, most patients endure frequent medical procedures, readmissions, and a diminished QoL.4,5 Additionally, recalcitrant wounds can lead to amputation.
Mechanical thrombectomy (MT) has emerged as a promising treatment option. By addressing the root cause — CVFO— cephalad flow may be restored using MT to accelerate delivery of mechanistic factors that promote wound healing (Figure 1). Recently, MT with the ClotTriever® system (Inari Medical) was shown to effectively treat acute-to-chronic material.6 In the 500-patient CLOUT registry, one-third presented with chronic disease, and results showed complete or near-complete thrombus removal in over 90% of patients, coupled with a >80% two-year PTS-free rate.
The potential of MT for CEAP-6 venous disease secondary to CVFO has been recently demonstrated.7,8 In a retrospective analysis of 11 CEAP-6 patients with 15 wounds in 14 limbs, CVFOs were successfully extirpated in all cases using MT–and when necessary, stenting and venoplasty–resulting in sustained vessel patency.8 Following comprehensive wound care management, 80% of wounds completely healed in 10 weeks. These promising results encourage future studies to validate the safety and long-term efficacy of this treatment paradigm.
Beyond the impact on patients’ well-being and QoL, open wounds impose a significant economic burden associated with recurrent inpatient and outpatient visits, treatments, homecare services, and hospitalization for infections. In the case of the CEAP-6 patients mentioned above, the cost of care, including an initial annual cost of $15K and increasing to $34K in cases of delayed healing,4 can amount to $3.5M, assuming an average of 10 years of treatment per patient. However, as reported, MT was an effective solution in these 11 cases, precluding the need for expenditures related to delayed healing. The cost would have decreased to $165K — a 95% reduction.Adopting such treatment strategies would alleviate the national economic burden associated with recalcitrant wounds.
We believe that the development of MT devices capable of clearing CVFOs heralds a transformative era in CVD management. Companies like Inari Medical are continually expanding their comprehensive toolkit including ClotTriever® BOLD, RevCore, and newly FDA-cleared VenaCore™ to treat native vessel and in-stent occlusions. A treatment paradigm consisting of MT and comprehensive wound care management9 may mitigate the devastating impact of CVD, enhancing patients’ QoL and curbing healthcare expenditures.
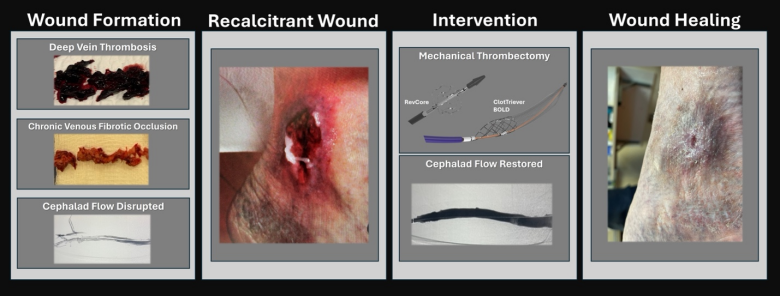
Figure 1: Summary of the proposed mechanism of promoting CEAP 6 wound healing via mechanical thrombectomy in CVD patients with recalcitrant wounds secondary to chronic venous fibrotic occlusions.
References
- Farrell JJ, Sutter C, Tavri S, Patel I. Incidence and interventions for post-thrombotic syndrome. Cardiovasc Diagn Ther. 2016;6(6):623-631.
- Bistervels IM, Bavalia R, Beyer-Westendorf J, Ten Cate-Hoek AJ, Schellong SM, Kovacs MJ, et al. Postthrombotic syndrome and quality of life after deep vein thrombosis in patients treated with edoxaban versus warfarin. Res Pract Thromb Haemost. 2022;6(5):e12748.
- Probst S, Saini C, Gschwind G, Stefanelli A, Bobbink P, Pugliese MT, et al. Prevalence and incidence of venous leg ulcers-A systematic review and meta-analysis. Int Wound J. 2023;20(9):3906-3921.
- Raffetto JD, Ligi D, Maniscalco R, Khalil RA, Mannello F. Why Venous Leg Ulcers Have Difficulty Healing: Overview on Pathophysiology, Clinical Consequences, and Treatment. J Clin Med. 2020;10(1)doi:10.3390/jcm10010029
- Bonkemeyer Millan S, Gan R, Townsend PE. Venous Ulcers: Diagnosis and Treatment. Am Fam Physician. 2019;100(5):298-305.
- Bisharat MB, Ichinose EJ, Veerina KK, Khetarpaul V, Azene EM, Plotnik AN, et al. One-Year Clinical Outcomes Following Mechanical Thrombectomy for Deep Vein Thrombosis: A CLOUT Registry Analysis. J Soc for Cardiovasc Angiography & Intervent. 2024;3(3):101307.
- Mouawad NJ. Percutaneous mechanical thrombectomy to remove post-thrombotic obstructions and manage post-thrombotic syndrome-associated venous leg ulceration. J Vasc Surg Venous Lymphat Disord. 2023;11(5):964-71.e1.
- Mouawad NJ. Chronic venous ulcer resolution and post-thrombotic syndrome improvement after percutaneous mechanical thrombectomy of a 42-year-old deep vein thrombosis. J Vasc Surg Cases Innov Tech.2022;8(2):196-200.
- Mouawad NJ. A referral pathway for treating patients with severe venous disease using mechanical thrombectomy. Wounds. 2024;36(4):115-118. doi:10.25270/wnds/23170
What Patients Are Saying About
JOBST® Compression Innovations

Margie Hopkins, BS, MHA
US Marketing Activation Manager
Essity
A recently published study in JOURNAL OF WOUND CARE VOL 33, NO 4, APRIL 2024 looks at the technologically advanced JOBST® Confidence garment. The aim of this study was to evaluate clinical performance, parameters related to quality of life (QoL) and patient satisfaction with innovative, made-to-measure, flat-knit compression garments for the daytime treatment of patients with leg or arm lymphoedema in their daily routine. This study was conducted at 4 locations in Germany over a 16-month period.
Compression therapy is considered the most important part of lymphoedema management. However, treatment adherence is crucial for ensuring successful therapy outcomes. Adherence is mainly affected by compression tolerability: poor choice of compression garment and its material can cause adverse effects, such as pain, discomfort, tightness, heat build-up under the garment, or skin irritation. Such effects were shown to be one of the main reasons for non-adherence. A survey among patients with lymphoedema revealed that 24% never wore their compression stockings. Therefore, new technologies are needed to improve product features that are crucial for good therapy adherence.
The JOBST® Confidence results in the study showed:
- 85% of study patients said they could move more freely in the JOBST® Confidence (with next generation technology like Contour Fit–an innovative knitting method that allows the garment to conform to individual’s body shapes)
- 92% of study patients agreed JOBST Confidence keeps the skin dry (an advanced moisture management system with double layer construction for optimal wearing comfort)
- 84% of patients evaluated the comfort of JOBST Confidence as good/very good
- 7 out of 10 of the study patients would recommend JOBST Confidence

Finding the right garment for patients is critical to the patient’s success. The Lymphedema Treatment Act will now give Medicare patients coverage that was not previously available to them. Every patient who needs compression should be able to get compression garments that are comfortable, containing, and fit their lifestyle.
To read the entire study please visit JCI from Essity – JOBST product & educational literature (jobstcompressioninstitute.com).
Bandage-Free Venous Leg Ulcer Treatment

Sundaram Ravikumar MD, MBBS, FRCS(C)
Vascular Surgeon
Westchester Vascular
Venous leg ulcers (VLUs) are the most common type of chronic wound, accounting for nearly 70% of lower extremity wounds. The prevalence of VLU is estimated to be about 4% of the population. Compression is the mainstay of therapy and aimed at edema reduction and improving hemodynamics to reduce venous hypertension, which improves wound healing and decreases recurrences.
Traditional inelastic multi-layer bandages have numerous limitations. They require appropriate training and placement is time-consuming. They require frequent changes for wounds with heavy exudate. For patients, it limits bathing, shoe choice, and leads to malodor.
Compliance with traditional compression solutions is low, with data estimating that nearly 60-70% of patients are non-compliant, especially with inelastic multi-layer bandages.
Sun Scientific has developed an effective and patient-focused solution, the AeroCare™ System, that incorporates the main therapies of effective VLU management: wound dressing, exudate management, and compression.
The wound dressing is fitted specifically to the patient’s wound to provide targeted coverage.
The exudate management component, ExuCare™, is a pre-shaped, superabsorbent dressing. The gelling effect helps to lock in fluid and keeps the skin dry even in a fully saturated dressing, thereby reducing the risk of skin breakdown. The reusable attachment tabs on the ExuCare allow wound inspection without having to remove the bandage and redress the wound.
Compression is achieved using the AeroWrap™, an inelastic, air-filled chamber with gradient compression. The AeroWrap™ is resuable, easy to apply, and has a hand-held pump that allows the patient and clinician to adjust pressures. It has a safety valve to avoid overinflation.


UnnaCare Wound Dressing

AeroBolster

AeroBolster

ExuCare dressing for exudate management

AeroWrap compression garment
The AeroCare™ system was applied on 4 patients with 5 with venous leg ulcers. All patients enrolled had chronic non-healing ulcers of > 1 year duration and had failed standard multi-layer bandage therapy.
|
Ulcer # |
Age |
Duration of Ulcer |
Size of Ulcer Week 0 (cm) |
Size of Ulcer Week 1 (cm) |
Size of Ulcer Week 2 (cm) |
Size of Ulcer Week 3 (cm) |
Size of Ulcer Week (cm) |
Size of Ulcer Week 5 (cm) |
|
#1 |
66 |
> 1 year |
9 x 5 (2/16) |
9 x 5 (2/21) |
6 x 3 (3/1) |
|
2 x 2 2 x 2 (3/13) |
|
|
#2 |
44 |
> 1 year |
10 x 6 x 6 (1/10) |
|
|
|
|
Completely healed |
|
#3 |
44 |
> 1 year |
7 x 7 (1/10) |
|
|
|
|
Completely healed |
|
#4 |
80 |
> 1 year |
3 x 2 x 1 (8/1) |
|
1 x 1 x 1 (8/14) |
|
Healed (8/29) |
|
|
#5 |
35 |
> 1 year |
3 x 4 (6/6) |
|
Completely healed (6/20) |
|
|

Week 0

Week 0

Week 1

Week 2

Week 4

Week 6

Week 7
This small pilot study shows that appropriate wound-healing can be achieved without traditional multi-layer bandaging.
